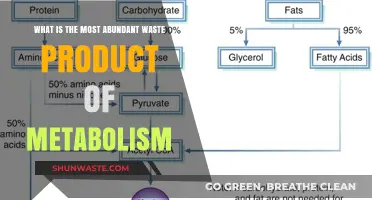
The human body continuously produces waste products as a result of metabolic processes, and one of the most significant among these is nitrogenous waste, which primarily arises from the breakdown of proteins and nucleic acids. Among the various nitrogenous compounds present in the blood, urea stands out as the most abundant, accounting for approximately 80-90% of the total nitrogenous waste. Produced in the liver through the urea cycle, urea is a highly soluble and non-toxic molecule that efficiently eliminates excess nitrogen from the body. Its prevalence in the bloodstream highlights its crucial role in maintaining nitrogen balance and preventing the accumulation of harmful ammonia, making it a key focus in understanding renal function and metabolic health.
| Characteristics | Values |
|---|---|
| Name | Urea |
| Chemical Formula | (NH₂)₂CO |
| Molecular Weight | 60.06 g/mol |
| Appearance | Colorless, crystalline solid |
| Solubility in Water | Highly soluble (110 g/100 mL at 20°C) |
| Production Site | Liver (via the urea cycle) |
| Primary Function | Excretion of excess nitrogen from protein metabolism |
| Normal Blood Concentration | 2.5 to 7.5 mg/dL (milligrams per deciliter) |
| Excretion Route | Kidneys (via urine) |
| Toxicity | Generally non-toxic at normal levels; high levels can cause uremia |
| Clinical Significance | Elevated levels may indicate kidney dysfunction, dehydration, or high protein intake |
| Role in Diagnosis | Used to assess kidney function (e.g., blood urea nitrogen, BUN test) |
| Environmental Impact | Major component of mammalian waste, affecting aquatic ecosystems |
| Industrial Uses | Fertilizer, resin production, and as a reagent in chemical synthesis |
Explore related products





What You'll Learn
- Urea Production: Liver converts ammonia to urea via the urea cycle, primary nitrogenous waste in blood
- Ammonia Toxicity: Ammonia is highly toxic; rapid conversion to urea prevents harm to tissues
- Urea Transport: Urea circulates in blood, filtered by kidneys, and excreted in urine
- Kidney Function: Kidneys regulate urea levels, ensuring balance and waste elimination
- Clinical Significance: Elevated blood urea indicates kidney dysfunction or dehydration, requiring medical attention
![]()
Urea Production: Liver converts ammonia to urea via the urea cycle, primary nitrogenous waste in blood
The liver is the body's primary detoxification center, and one of its critical functions is converting toxic ammonia into urea, a less harmful nitrogenous waste. This process, known as the urea cycle, is essential for maintaining nitrogen balance and preventing ammonia toxicity, which can be fatal even at low concentrations. Understanding this mechanism not only highlights the liver's role in metabolic health but also underscores the significance of urea as the most abundant nitrogenous waste in the blood.
The Urea Cycle: A Step-by-Step Breakdown
The urea cycle involves a series of biochemical reactions that occur primarily in the liver. It begins with the combination of ammonia (NH₃), produced from protein metabolism, and carbon dioxide (CO₂) to form carbamoyl phosphate. This intermediate then reacts with ornithine to produce citrulline, which is transported to the mitochondria. There, citrulline combines with aspartate to form argininosuccinate, which is cleaved into arginine and fumarate. Finally, arginine is hydrolyzed into urea and ornithine, completing the cycle. Each step is catalyzed by specific enzymes, such as ornithine transcarbamylase and arginase, whose deficiencies can lead to rare but severe metabolic disorders.
Ammonia is highly toxic, particularly to the brain, where it disrupts neuronal function and can cause encephalopathy. By converting ammonia to urea, the liver reduces its toxicity by a factor of 100, making it safe for transport in the blood to the kidneys for excretion. Urea is also more soluble in water, facilitating its elimination in urine. This transformation is a prime example of the body’s ability to repurpose waste into a form that minimizes harm while efficiently removing excess nitrogen.
Practical Implications and Health Considerations
For individuals with liver disease, such as cirrhosis or hepatitis, the urea cycle can be compromised, leading to elevated ammonia levels and potential hepatic encephalopathy. Symptoms may include confusion, lethargy, and in severe cases, coma. Management often involves dietary modifications, such as reducing protein intake to limit ammonia production, and medications like lactulose, which acidifies the gut to trap ammonia. Monitoring blood urea nitrogen (BUN) levels is a common clinical practice to assess liver and kidney function, with normal ranges typically between 7 to 20 mg/dL in adults.
Comparative Perspective: Urea vs. Other Nitrogenous Wastes
While urea is the primary nitrogenous waste in mammals, other organisms handle nitrogen differently. Birds and reptiles excrete nitrogen as uric acid, which is less soluble but more compact, conserving water in arid environments. In contrast, fish excrete ammonia directly, relying on their aquatic habitat to dilute its toxicity. This diversity highlights the evolutionary adaptation of nitrogen waste management across species, with urea production in humans being a finely tuned process optimized for our physiological needs.
In summary, the liver’s role in converting ammonia to urea via the urea cycle is a cornerstone of metabolic health, ensuring the safe elimination of nitrogenous waste. Understanding this process not only sheds light on the body’s intricate detoxification mechanisms but also emphasizes the importance of maintaining liver function for overall well-being. Whether through dietary adjustments or medical interventions, supporting this vital pathway is key to preventing complications associated with nitrogen imbalance.
Sustainable Construction: Effective Recycling Strategies for On-Site Waste Management
You may want to see also
Explore related products






![]()
Ammonia Toxicity: Ammonia is highly toxic; rapid conversion to urea prevents harm to tissues
Ammonia, a byproduct of protein metabolism, is the most abundant nitrogenous waste in the blood. While essential for cellular processes, it becomes highly toxic at elevated levels, posing a significant threat to tissues, particularly the brain. Even a slight increase in blood ammonia concentration can disrupt neurological function, leading to symptoms like confusion, lethargy, and in severe cases, coma. This toxicity arises from ammonia’s ability to interfere with ATP production, alter neurotransmitter balance, and increase oxidative stress, making its rapid removal critical for survival.
The body employs a sophisticated detoxification mechanism centered on the urea cycle, primarily occurring in the liver. This cycle converts ammonia into urea, a far less toxic compound that can be safely excreted in urine. The process begins with the combination of ammonia and carbon dioxide to form carbamoyl phosphate, which is then converted to citrulline and eventually urea. Key enzymes like carbamoyl phosphate synthetase, ornithine transcarbamylase, and arginase play pivotal roles in this pathway. Without this rapid conversion, ammonia would accumulate, causing irreversible damage to the central nervous system and other organs.
Certain conditions, such as liver failure or genetic defects in the urea cycle, can impair ammonia detoxification, leading to hyperammonemia. For instance, individuals with ornithine transcarbamylase deficiency, a rare genetic disorder, are unable to efficiently convert ammonia to urea, resulting in toxic buildup. In such cases, immediate medical intervention is necessary, often involving medications like sodium benzoate or arginine, which help bind ammonia and promote its excretion. Dietary modifications, such as reducing protein intake, are also crucial to managing ammonia levels in these patients.
Understanding ammonia toxicity underscores the importance of maintaining a functional urea cycle and liver health. Regular monitoring of ammonia levels is essential for individuals at risk, including those with liver disease or inherited metabolic disorders. Early detection and intervention can prevent severe complications, such as hepatic encephalopathy, a condition characterized by brain dysfunction due to ammonia accumulation. By appreciating the delicate balance between ammonia production and its detoxification, healthcare providers can better manage patients and mitigate the risks associated with this toxic waste product.
Cnidarian Nitrogen Waste Removal: Strategies for Efficient Detoxification
You may want to see also
Explore related products






![]()
Urea Transport: Urea circulates in blood, filtered by kidneys, and excreted in urine
Urea, a byproduct of protein metabolism, is the most abundant nitrogenous waste in the blood, accounting for approximately 80-90% of the total nitrogenous waste excreted by the body. Its presence is a natural consequence of the breakdown of amino acids, primarily occurring in the liver through the urea cycle. This process converts toxic ammonia, a byproduct of amino acid deamination, into urea, which is far less harmful and can be safely transported in the bloodstream.
The Journey of Urea: A Transport Perspective
Imagine a bustling highway system, but instead of cars, it's urea molecules traveling through your body. After its production in the liver, urea enters the bloodstream, where it's carried to the kidneys. This transport is passive, meaning it doesn't require energy expenditure. The concentration gradient between the blood and the kidneys drives the movement of urea, ensuring its efficient delivery for filtration.
Filtration and Reabsorption: A Delicate Balance
Upon reaching the kidneys, urea faces a crucial juncture. The glomeruli, tiny filters within the kidneys, allow small molecules like urea to pass through into the nephron tubules. However, unlike other waste products, a significant portion of urea (about 40-50%) is reabsorbed back into the bloodstream as it travels through the proximal tubule. This reabsorption is not a mistake; it's a carefully regulated process that helps maintain the body's urea balance and prevents excessive loss.
Excretion: The Final Leg of the Journey
The remaining urea, along with other waste products and excess water, continues its journey through the nephron tubules, eventually reaching the collecting ducts. Here, the final concentration of urine is adjusted based on the body's hydration status. Urea, being highly soluble, remains dissolved in the urine and is ultimately excreted from the body during urination. This process completes the cycle, removing waste products and maintaining the body's internal equilibrium.
Practical Implications: When Urea Transport Goes Awry
Understanding urea transport is crucial in diagnosing and managing kidney disorders. Elevated blood urea nitrogen (BUN) levels can indicate kidney dysfunction, as impaired filtration leads to urea accumulation. Conversely, conditions like liver disease can disrupt urea production, resulting in low BUN levels. Monitoring BUN levels, along with other markers, provides valuable insights into kidney health and overall metabolic function.
Prevent Muscle Atrophy Post-Knee Surgery: Effective Strategies for Recovery
You may want to see also
Explore related products





![]()
Kidney Function: Kidneys regulate urea levels, ensuring balance and waste elimination
Urea, a byproduct of protein metabolism, stands as the most abundant nitrogenous waste in the blood. It forms when the liver breaks down excess amino acids and ammonia, a process crucial for detoxifying the body. However, its presence in excessive amounts can be harmful, leading to symptoms like fatigue, nausea, and confusion. This is where the kidneys step in, playing a pivotal role in maintaining urea levels within a safe range, typically between 6 to 20 mg/dL in adults.
The kidneys achieve this regulation through a meticulous filtration and reabsorption process. Blood enters the kidneys and is filtered through tiny structures called nephrons. Here, urea, along with other waste products and excess water, is separated from essential substances like glucose and amino acids. Interestingly, unlike some other waste products, urea is not actively secreted by the kidneys. Instead, its excretion is primarily driven by the concentration gradient, meaning the kidneys allow it to passively pass into the urine. This process is finely tuned to ensure that the body retains enough nitrogen for vital functions while eliminating the excess.
Practical Tip: Staying adequately hydrated is crucial for optimal kidney function and urea excretion. Aim for 8-10 cups of water daily, adjusting based on activity level and climate.
While the kidneys are highly efficient, certain factors can disrupt their ability to regulate urea levels. Dehydration, for example, concentrates urea in the blood, leading to elevated levels. Conversely, overhydration can dilute urea, potentially masking underlying kidney dysfunction. Caution: Individuals with kidney disease often experience impaired urea clearance, leading to a condition called uremia, characterized by dangerously high urea levels. Symptoms include loss of appetite, itching, and difficulty concentrating.
Takeaway: Monitoring urea levels through regular blood tests is essential for individuals at risk of kidney problems, including those with diabetes, high blood pressure, or a family history of kidney disease.
Understanding the kidneys' role in urea regulation highlights the importance of maintaining kidney health. A balanced diet low in processed foods and excessive protein, regular exercise, and managing underlying health conditions are key preventive measures. By appreciating the intricate dance between urea production and kidney function, we can take proactive steps to ensure our bodies effectively eliminate waste and maintain overall well-being.
Mincer Attachment for Waste Tacks: Uses, Benefits, and How It Works
You may want to see also
Explore related products





![]()
Clinical Significance: Elevated blood urea indicates kidney dysfunction or dehydration, requiring medical attention
Urea, a byproduct of protein metabolism, is the most abundant nitrogenous waste in the blood, accounting for approximately 90% of the total nitrogenous waste excreted by the kidneys. It is produced in the liver through the urea cycle, which converts toxic ammonia into urea, a less harmful substance that can be safely eliminated through urine. Under normal circumstances, blood urea levels remain stable, reflecting a balance between production and excretion. However, elevated blood urea levels, a condition known as hyperuremia, serve as a critical clinical marker that demands immediate attention.
Analytical Perspective: Elevated blood urea levels are not merely a laboratory finding but a symptom of underlying physiological disturbances. The kidneys, responsible for filtering urea from the blood, play a central role in maintaining urea homeostasis. When kidney function declines—whether due to acute kidney injury (AKI), chronic kidney disease (CKD), or obstructive uropathy—urea clearance decreases, leading to its accumulation in the blood. Dehydration exacerbates this process by reducing blood flow to the kidneys, further impairing their ability to excrete urea. Clinicians must interpret elevated urea levels in conjunction with other markers, such as creatinine and electrolyte levels, to differentiate between prerenal (e.g., dehydration) and intrinsic renal causes (e.g., glomerulonephritis).
Instructive Approach: Patients with elevated blood urea levels should undergo a thorough evaluation to identify the root cause. For dehydration, immediate rehydration is essential, often achieved through oral fluid intake or intravenous fluids, depending on severity. In cases of kidney dysfunction, treatment may involve addressing the underlying condition—for instance, managing hypertension in CKD or removing obstructions in uropathy. Monitoring blood urea nitrogen (BUN) levels is crucial, with normal ranges typically between 6 to 20 mg/dL. Values exceeding 20 mg/dL warrant investigation, while levels above 50 mg/dL indicate severe impairment requiring urgent intervention.
Persuasive Argument: Ignoring elevated blood urea levels can have dire consequences. Chronic hyperuremia is associated with uremic syndrome, a life-threatening condition characterized by symptoms like nausea, confusion, and seizures. In older adults, particularly those over 65, elevated urea levels may exacerbate cognitive decline and increase mortality risk. Early detection and management are paramount. Patients with risk factors—such as diabetes, hypertension, or a history of kidney disease—should undergo regular renal function tests. Lifestyle modifications, including a low-protein diet and adequate hydration, can help mitigate risks, but medical supervision is indispensable.
Comparative Insight: While elevated blood urea is a reliable indicator of kidney dysfunction or dehydration, it is not specific to these conditions. Other factors, such as high-protein diets, gastrointestinal bleeding, or certain medications (e.g., steroids), can also elevate urea levels. For instance, athletes on high-protein regimens may exhibit transient hyperuremia without underlying renal issues. Conversely, low urea levels, though less common, may indicate liver disease or malnutrition. Clinicians must contextualize urea levels within the patient’s overall health profile to avoid misdiagnosis.
Practical Takeaway: Elevated blood urea levels are a red flag that should never be overlooked. For individuals, staying hydrated and maintaining a balanced diet are simple yet effective preventive measures. For healthcare providers, a systematic approach—including history-taking, physical examination, and laboratory testing—is essential for accurate diagnosis and timely intervention. In both scenarios, vigilance and proactive management can prevent complications and improve outcomes, underscoring the clinical significance of this vital biomarker.
Transform Organic Waste into Profit: Sustainable Income Strategies Revealed
You may want to see also
Frequently asked questions
The most abundant nitrogenous waste in the blood is urea.
Urea is produced in the liver through the urea cycle (also known as the ornithine cycle), which converts toxic ammonia, a byproduct of protein metabolism, into urea for safe excretion.
Urea is the primary nitrogenous waste in humans because it is less toxic than ammonia and more soluble than uric acid, making it easier to excrete through urine while minimizing harm to the body.