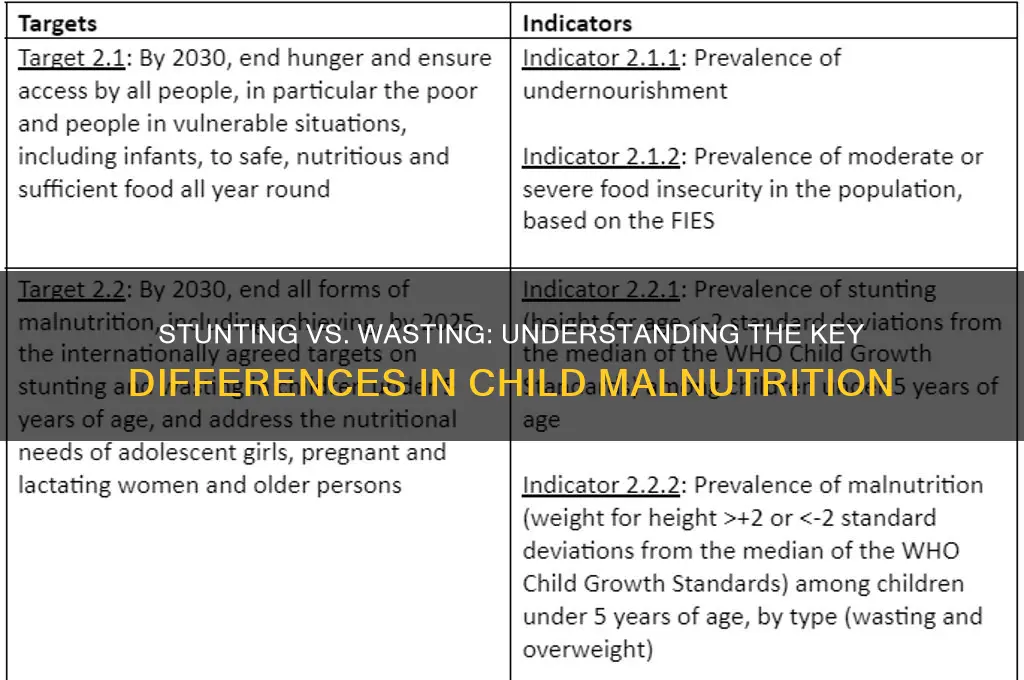
Stunting and wasting are both forms of malnutrition, but they represent distinct conditions with different causes and implications. Stunting refers to impaired growth and development in children, characterized by a low height-for-age ratio, and is typically the result of chronic or long-term malnutrition, poor maternal health, and inadequate access to nutritious food and healthcare. It often leads to irreversible physical and cognitive developmental delays. In contrast, wasting is a severe and acute form of malnutrition marked by a low weight-for-height ratio, indicating rapid weight loss or failure to gain weight. It is usually caused by recent food shortages, illness, or insufficient nutrient intake and poses an immediate threat to a child’s life if left untreated. While stunting reflects long-term deprivation, wasting highlights an urgent need for intervention to prevent mortality and restore health. Understanding these differences is crucial for designing targeted nutrition and health programs to address each condition effectively.
| Characteristics | Values |
|---|---|
| Definition | Stunting: Impaired growth and development due to chronic malnutrition, typically measured as height-for-age <-2 Z-score. Wasting: Acute weight loss or failure to gain weight due to recent rapid weight loss or lack of weight gain, typically measured as weight-for-height <-2 Z-score. |
| Cause | Stunting: Prolonged insufficient nutrient intake, poor socioeconomic conditions, and recurrent infections. Wasting: Recent acute food shortage, illness, or a combination of both. |
| Timeframe | Stunting: Develops over months or years, reflecting long-term nutritional deficiencies. Wasting: Develops over weeks or months, indicating recent nutritional stress. |
| Prevalence | Stunting: More common in low- and middle-income countries, affecting approximately 149 million children under 5 (2021 data). Wasting: Globally, around 45 million children under 5 were wasted in 2021, with higher prevalence in humanitarian crises. |
| Health Impact | Stunting: Irreversible damage to cognitive and physical development, increased risk of chronic diseases in adulthood. Wasting: Immediate life-threatening risk, increased susceptibility to infections, and higher mortality rates. |
| Measurement | Stunting: Height-for-age Z-score (HAZ) <-2 SD from WHO Child Growth Standards. Wasting: Weight-for-height Z-score (WHZ) <-2 SD or mid-upper arm circumference (MUAC) < 115 mm. |
| Reversibility | Stunting: Largely irreversible after age 2-3, though some catch-up growth is possible. Wasting: Reversible with appropriate nutritional intervention and treatment of underlying causes. |
| Intervention | Stunting: Focus on long-term strategies like improving maternal nutrition, sanitation, and access to healthcare. Wasting: Requires immediate therapeutic feeding programs and medical treatment for underlying conditions. |
| Global Targets | Stunting: WHO aims to reduce prevalence by 40% by 2025 (from 2010 baseline). Wasting: Global target to reduce and maintain childhood wasting to <5% by 2025. |
Explore related products






What You'll Learn
- Definition of Stunting: Chronic malnutrition, impaired growth, height-for-age below WHO standards, long-term effects
- Definition of Wasting: Acute malnutrition, rapid weight loss, weight-for-height below WHO standards, immediate risk
- Causes of Stunting: Prolonged poor nutrition, recurrent infections, inadequate care, early childhood deprivation
- Causes of Wasting: Sudden food shortage, illness, conflict, or displacement, short-term nutritional crisis
- Health Implications: Stunting affects cognitive development; wasting increases mortality risk, both require urgent intervention
![]()
Definition of Stunting: Chronic malnutrition, impaired growth, height-for-age below WHO standards, long-term effects
Stunting, a silent yet pervasive condition, affects millions of children globally, leaving an indelible mark on their physical and cognitive development. It is a form of chronic malnutrition that occurs when a child's height-for-age is significantly below the World Health Organization (WHO) standards. This condition is not merely about being short; it is a complex health issue with far-reaching consequences. The WHO defines stunting as a height-for-age Z-score of less than -2 standard deviations from the median of the WHO Child Growth Standards. In simpler terms, it means a child is too short for their age, indicating a long-term failure to receive adequate nutrition.
The causes of stunting are multifaceted, often rooted in a combination of poor dietary intake, frequent infections, and inadequate care practices during the first 1,000 days of life, from conception to a child's second birthday. This critical period lays the foundation for a child's future health and development. For instance, a mother's nutrition during pregnancy directly impacts the baby's growth, and breastfeeding practices in the early months are crucial for providing essential nutrients. Insufficient access to nutritious foods, such as those rich in proteins, vitamins, and minerals, can lead to a child's body not receiving the necessary building blocks for growth.
The effects of stunting extend far beyond physical appearance. It is associated with impaired cognitive development, reduced school performance, and lower economic productivity in adulthood. Stunted children are more likely to suffer from chronic diseases later in life, such as diabetes and cardiovascular problems. The impact on brain development is particularly concerning, as it can lead to irreversible damage, affecting a child's ability to learn and reach their full potential. For example, studies have shown that stunted children often score lower on cognitive tests and are more likely to repeat grades in school.
Addressing stunting requires a multi-pronged approach. Firstly, ensuring adequate nutrition during pregnancy and early childhood is paramount. This includes promoting diverse and nutrient-rich diets, such as foods fortified with vitamins and minerals, especially in communities where access to fresh produce is limited. Secondly, improving sanitation and hygiene practices can reduce the burden of infections, which often exacerbate malnutrition. Educating caregivers about proper feeding practices, such as exclusive breastfeeding for the first six months and timely introduction of complementary foods, is essential.
In conclusion, stunting is a critical global health issue that demands attention and action. By understanding its definition, causes, and long-term effects, we can implement targeted interventions to prevent and treat this condition. The focus should be on providing practical solutions, such as community-based nutrition programs, education initiatives, and policies that improve food security and access to healthcare. Early intervention is key, as the first few years of life present a unique window of opportunity to shape a child's future health and well-being.
Easy Guide to Installing a Pop-Up Waste in Your Sink
You may want to see also
Explore related products

$39.99 $49.99





![]()
Definition of Wasting: Acute malnutrition, rapid weight loss, weight-for-height below WHO standards, immediate risk
Wasting, a stark indicator of acute malnutrition, manifests as a rapid and severe decline in a child’s weight relative to their height, falling below the World Health Organization (WHO) standards. This condition is not merely a number on a growth chart; it signals an immediate threat to a child’s survival. Unlike stunting, which develops over time due to chronic malnutrition, wasting is a crisis that demands urgent attention. It often arises from sudden food shortages, illness, or inadequate feeding practices, leaving children dangerously vulnerable to life-threatening complications.
To identify wasting, health workers measure a child’s mid-upper arm circumference (MUAC) or assess their weight-for-height Z-score (WHZ). A MUAC below 115 mm or a WHZ below -2 indicates severe acute malnutrition (SAM), the most critical form of wasting. These metrics are not just clinical tools; they are alarms that prompt immediate intervention. For instance, a child with SAM is 11 times more likely to die compared to a well-nourished child, underscoring the urgency of addressing this condition.
Practical steps to combat wasting include therapeutic feeding programs, which provide nutrient-dense foods like ready-to-use therapeutic food (RUTF). RUTF, a peanut-based paste fortified with vitamins and minerals, is designed to rapidly restore a child’s weight and health. Alongside nutrition, treating underlying infections with antibiotics and ensuring access to clean water are critical. Parents and caregivers play a vital role by monitoring feeding patterns and seeking medical help at the first sign of rapid weight loss or illness.
While wasting is reversible with timely intervention, prevention is equally crucial. Educating communities about proper infant and young child feeding practices, such as exclusive breastfeeding for the first six months and timely introduction of complementary foods, can reduce the risk. Early detection through routine growth monitoring and screening at health facilities ensures that children receive treatment before their condition deteriorates. Wasting is not just a health issue; it is a call to action to address the immediate and underlying causes of malnutrition.
In summary, wasting is a severe, acute form of malnutrition characterized by rapid weight loss and a weight-for-height measurement below WHO standards. It poses an immediate risk to a child’s life, requiring swift and targeted interventions. By understanding its causes, recognizing its signs, and implementing evidence-based solutions, we can save lives and prevent the devastating consequences of this condition. Wasting is a crisis, but it is also an opportunity to act decisively and make a tangible difference in a child’s future.
Transforming Trash into Treasure: Innovative Science-Based Waste Upcycling Ideas
You may want to see also
Explore related products





![]()
Causes of Stunting: Prolonged poor nutrition, recurrent infections, inadequate care, early childhood deprivation
Stunting, a condition marked by impaired growth and development in children, is primarily driven by four interconnected factors: prolonged poor nutrition, recurrent infections, inadequate care, and early childhood deprivation. Unlike wasting, which reflects acute malnutrition and recent weight loss, stunting is a chronic issue that manifests over time, often irreversible after the first 1,000 days of life. Understanding these causes is crucial for targeted interventions, as stunting affects not only physical growth but also cognitive function, immune response, and long-term productivity.
Prolonged poor nutrition is the cornerstone of stunting. Children require a balanced intake of macronutrients (proteins, fats, carbohydrates) and micronutrients (iron, zinc, vitamin A) for optimal growth. For instance, a diet deficient in protein leads to muscle wasting, while inadequate vitamin A intake weakens the immune system, increasing susceptibility to infections. In low-income settings, staple foods like rice or maize often dominate diets, lacking essential nutrients. Practical solutions include diversifying diets with locally available nutrient-rich foods, such as leafy greens, legumes, and fortified staples. For children under two, the World Health Organization recommends exclusive breastfeeding for the first six months, followed by complementary feeding with nutrient-dense foods to meet daily requirements of 500–600 kcal and 10–15g of protein.
Recurrent infections, particularly diarrheal diseases and respiratory infections, exacerbate stunting by diverting nutrients away from growth and toward immune responses. Each episode of diarrhea can reduce nutrient absorption by up to 50%, creating a vicious cycle of malnutrition and illness. For example, in regions with poor sanitation, children may experience 4–8 diarrheal episodes annually, each depleting essential nutrients like zinc and potassium. Preventive measures include improving access to clean water, promoting handwashing, and administering vaccines for rotavirus and pneumonia. Zinc supplementation (20 mg/day for 10–14 days during diarrhea) and oral rehydration solutions can mitigate nutrient loss and reduce severity.
Inadequate care encompasses both physical and emotional neglect, which hinder growth by disrupting hormonal and metabolic processes. For instance, children who lack responsive caregiving often experience elevated cortisol levels, a stress hormone that impairs growth hormone secretion. In orphanages or overcrowded households, children may receive insufficient attention, leading to poor feeding practices and delayed developmental milestones. Caregiver training programs that emphasize responsive feeding, hygiene, and stimulation can significantly reduce stunting rates. For example, the Care for Child Development program by UNICEF integrates nutrition education with play-based activities to foster healthy growth.
Early childhood deprivation, particularly in the first 1,000 days, has lifelong consequences. During this critical window, the brain undergoes rapid development, requiring adequate nutrition and stimulation. Children deprived of essential nutrients or nurturing environments during this period often face irreversible cognitive and physical deficits. For example, iron deficiency anemia in infancy, affecting 40% of children globally, is linked to reduced IQ scores and poorer school performance. Interventions like prenatal folic acid supplementation (400 µg/day) and early childhood education programs can mitigate these risks. Governments and NGOs must prioritize policies that support maternal health, breastfeeding, and access to nutritious foods during this pivotal stage.
Addressing stunting requires a multi-faceted approach that tackles its root causes. By improving dietary diversity, preventing infections, enhancing caregiving practices, and prioritizing early childhood development, communities can break the cycle of malnutrition and ensure children reach their full potential. Each intervention, no matter how small, contributes to a larger impact, transforming lives and shaping healthier futures.
Labor Day Waste Collection: Does Western Services Operate as Usual?
You may want to see also
Explore related products





![]()
Causes of Wasting: Sudden food shortage, illness, conflict, or displacement, short-term nutritional crisis
Wasting, a form of acute malnutrition, is characterized by a rapid decline in weight-for-height, often accompanied by visible signs like a gaunt face, protruding ribs, and loose skin. Unlike stunting, which is a chronic condition resulting from long-term nutritional deficiencies, wasting is a short-term crisis that demands immediate attention. It primarily affects children under five, with severe cases increasing the risk of mortality by up to 11 times compared to well-nourished peers. Understanding its causes is crucial for prevention and intervention.
Sudden food shortages, whether due to drought, economic collapse, or supply chain disruptions, are a leading trigger of wasting. For instance, in regions reliant on rain-fed agriculture, a failed harvest can leave families without access to staple foods for months. In such scenarios, children’s dietary intake plummets, often limited to one meal a day consisting of low-nutrient foods like porridge or bread. Practical tips for households include diversifying crops to include drought-resistant varieties like sorghum or millet and storing surplus food during bountiful seasons. Humanitarian aid organizations can mitigate this by distributing high-energy biscuits or ready-to-use therapeutic foods (RUTFs), which provide 500–550 kcal and essential micronutrients per 92-gram sachet.
Illness exacerbates wasting by reducing nutrient absorption and increasing metabolic demands. Diarrhea, pneumonia, and malaria are common culprits, particularly in areas with poor sanitation and limited access to healthcare. For example, a child with diarrhea loses critical electrolytes and nutrients, further depleting their already fragile nutritional status. Parents should prioritize hygiene practices like handwashing with soap and ensure children are fully vaccinated. In severe cases, oral rehydration salts (ORS) combined with zinc supplementation (20 mg/day for 10–14 days) can reduce the duration and severity of diarrhea, preventing the slide into wasting.
Conflict and displacement uproot families, severing their access to food, clean water, and healthcare. In refugee camps, overcrowding and inadequate resources create a breeding ground for malnutrition. For instance, during the Syrian conflict, displacement led to a 20% increase in wasting rates among children under five. Aid agencies must prioritize setting up nutrition clinics in camps, providing RUTFs, and establishing breastfeeding support programs for infants. Families can protect young children by carrying nutrient-dense foods like nuts or dried fruits during flight and seeking out nutrition screenings upon arrival.
Ultimately, wasting is a preventable crisis rooted in sudden, short-term shocks. Addressing it requires a multi-pronged approach: strengthening food systems, improving healthcare access, and providing rapid humanitarian response during conflicts or disasters. By focusing on these causes, we can safeguard children’s immediate survival and long-term health, ensuring wasting remains a temporary setback rather than a death sentence.
Eco-Friendly Ways to Dispose of Green Waste Effectively and Sustainably
You may want to see also
Explore related products






![]()
Health Implications: Stunting affects cognitive development; wasting increases mortality risk, both require urgent intervention
Stunting and wasting, though both indicators of malnutrition, diverge sharply in their health implications, demanding tailored interventions. Stunting, characterized by low height-for-age, primarily stems from chronic malnutrition and recurrent infections during the first 1,000 days of life. Its most insidious effect lies in impaired cognitive development. Studies show that stunted children score 7–15 points lower on IQ tests and are 19% less likely to read by age 8. This cognitive deficit translates to reduced school performance, lower wages in adulthood, and diminished economic productivity. For instance, a World Bank analysis estimates that stunting costs low- and middle-income countries up to 10% of their GDP annually. Interventions must focus on pregnant women and children under 2, emphasizing micronutrient supplementation (e.g., vitamin A, iron, iodine) and infection prevention through vaccination and sanitation.
Contrastingly, wasting, defined as low weight-for-height, is an acute condition often triggered by sudden food shortages, illness, or inadequate feeding practices. Its most immediate threat is heightened mortality risk, particularly in children under 5. Wasted children are 12 times more likely to die from common infections like diarrhea or pneumonia due to weakened immune systems. Alarmingly, severe wasting (weight-for-height < -3 z-scores) claims over 1 million young lives annually. Treatment protocols, such as the World Health Organization’s F-100 therapeutic food (a high-energy, micronutrient-rich peanut paste), have proven effective, with 85–90% recovery rates when administered promptly. Community health workers play a critical role in early detection through mid-upper arm circumference (MUAC) measurements, a simple yet powerful tool for identifying at-risk children.
While stunting’s cognitive impacts are irreversible after age 5, wasting’s mortality risk can be mitigated with swift action. This distinction underscores the urgency of dual-pronged strategies: long-term prevention for stunting (e.g., maternal nutrition programs, breastfeeding promotion) and rapid response systems for wasting (e.g., emergency food aid, decentralized treatment centers). Both conditions, however, share a common root in poverty and inequity, necessitating multisectoral approaches that address food insecurity, healthcare access, and education.
A compelling example is Ethiopia’s Seqota Declaration, which integrates stunting reduction with climate resilience initiatives, halving stunting rates in some regions within five years. Similarly, India’s POSHAN Abhiyaan uses real-time data tracking to target high-burden districts, coupling nutrition education with social safety nets. Such models illustrate that while stunting and wasting differ in manifestation, their solutions converge on equity, scalability, and political will.
Ultimately, the health implications of stunting and wasting are not merely medical but societal, perpetuating cycles of poverty unless addressed comprehensively. Policymakers, healthcare providers, and communities must recognize that stunting steals potential, while wasting steals lives—both demand urgent, context-specific action. As the global community strives to meet Sustainable Development Goal 2 (Zero Hunger), prioritizing these conditions is not just a moral imperative but a strategic investment in humanity’s future.
Eco-Friendly Solutions: Reusing RO Waste Water Effectively at Home
You may want to see also
Frequently asked questions
Stunting refers to impaired growth and development, characterized by low height-for-age, often due to chronic malnutrition. Wasting refers to acute malnutrition, characterized by low weight-for-height, typically caused by recent rapid weight loss or failure to gain weight.
Stunting is primarily caused by long-term insufficient nutrient intake, poor maternal nutrition, and recurrent infections. Wasting is usually caused by sudden food shortages, illness, or inadequate feeding practices over a short period.
Yes, a child can experience both conditions simultaneously, especially in severe cases of malnutrition where chronic undernutrition (stunting) is compounded by acute weight loss (wasting).
Stunting prevention focuses on long-term interventions like improving maternal nutrition, breastfeeding, and access to nutritious foods. Wasting treatment often involves therapeutic feeding programs and addressing immediate causes like infections. Prevention for both includes improving food security, healthcare, and sanitation.































