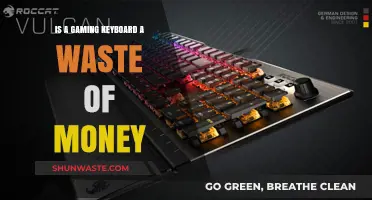
The question of whether a metabolic waste product results from protein metabolism is a fundamental concept in biochemistry. When proteins are broken down in the body, they undergo a series of metabolic processes, primarily in the liver, to produce energy and essential molecules. However, this breakdown also generates waste products, such as urea, which is a key example of a metabolic waste product resulting from protein metabolism. Urea is formed through the urea cycle, a series of biochemical reactions that convert toxic ammonia, produced during protein catabolism, into a less harmful substance that can be excreted by the kidneys. Understanding this process is crucial, as it highlights the body's efficient mechanism for managing waste while maintaining homeostasis. Platforms like Quizlet often provide educational resources to help students grasp these complex metabolic pathways, making it easier to comprehend how protein metabolism is intricately linked to waste production and elimination.
| Characteristics | Values |
|---|---|
| Name | Urea |
| Chemical Formula | CO(NH₂)₂ |
| Molecular Weight | 60.06 g/mol |
| Production Site | Liver (via the urea cycle) |
| Primary Function | Excretion of excess nitrogen from protein metabolism |
| Solubility | Highly soluble in water |
| Excretion Route | Kidneys (via urine) |
| Normal Blood Level | 6-20 mg/dL (milligrams per deciliter) |
| Increased Levels (Uremia) | Kidney disease, dehydration, high protein intake |
| Clinical Significance | Indicator of kidney function, metabolic disorders |
Explore related products






What You'll Learn
- Urea Production Pathway: How the liver converts ammonia into urea via the urea cycle
- Ammonia Toxicity: Why excess ammonia is harmful and must be converted to urea
- Urea Excretion: Role of kidneys in filtering and eliminating urea through urine
- Protein Metabolism Link: Breakdown of amino acids producing ammonia as a byproduct
- Urea Cycle Disorders: Genetic conditions disrupting urea production and causing ammonia buildup
![]()
Urea Production Pathway: How the liver converts ammonia into urea via the urea cycle
Protein metabolism generates ammonia, a highly toxic substance that must be neutralized and eliminated. The liver orchestrates this detoxification through the urea cycle, a complex metabolic pathway converting ammonia into urea, a far less harmful compound excreted in urine. This process is vital for maintaining nitrogen balance and preventing ammonia-induced brain damage.
Understanding the Urea Cycle:
Imagine a multi-step assembly line within liver cells. Ammonia, primarily from protein breakdown, enters the cycle. Through a series of enzymatic reactions, it combines with carbon dioxide and other molecules, ultimately forming urea. This urea is then transported to the kidneys for excretion.
Key Players in the Cycle:
Several enzymes act as catalysts, each playing a crucial role. Carbamoyl phosphate synthetase I (CPS1) initiates the cycle by combining ammonia with carbon dioxide. Ornithine transcarbamylase (OTC) and argininosuccinate synthetase (ASS) facilitate subsequent steps, leading to the formation of arginine. Finally, arginase splits arginine into urea and ornithine, which re-enters the cycle.
Clinical Significance:
Defects in urea cycle enzymes can lead to devastating disorders like ornithine transcarbamylase deficiency. These conditions result in ammonia accumulation, causing neurological damage, coma, and even death. Early diagnosis and treatment, often involving dietary restrictions and medications to lower ammonia levels, are crucial for managing these rare but serious conditions.
Practical Implications:
Understanding the urea cycle highlights the importance of a balanced diet. Excessive protein intake can overwhelm the cycle, potentially leading to increased ammonia production. Individuals with liver disease or urea cycle disorders require careful dietary management to prevent complications.
Muscles and Intestinal Waste Movement: How They Work Together
You may want to see also
Explore related products




![]()
Ammonia Toxicity: Why excess ammonia is harmful and must be converted to urea
Ammonia, a byproduct of protein metabolism, is inherently toxic to the body, particularly to the brain and other organs. When proteins are broken down, amino acids release ammonia (NH₃) as a waste product. While the body can tolerate small amounts, excess ammonia disrupts cellular function by altering pH balance and damaging tissues. For instance, elevated ammonia levels in the brain interfere with neurotransmitter synthesis and energy metabolism, leading to symptoms like confusion, lethargy, and, in severe cases, coma. This toxicity underscores the critical need for efficient ammonia detoxification, primarily through its conversion to urea.
The liver plays a central role in ammonia detoxification via the urea cycle, a series of biochemical reactions that convert ammonia into urea, a less toxic substance excreted in urine. This process begins with the combination of ammonia and carbon dioxide to form carbamoyl phosphate, which is then converted to urea through a series of enzyme-catalyzed steps. However, the urea cycle’s efficiency depends on adequate nutrient intake, particularly arginine and ornithine, which act as substrates. Individuals with liver disease or genetic disorders affecting the urea cycle are at higher risk of ammonia toxicity, as their bodies struggle to convert ammonia to urea effectively.
Excess ammonia is particularly dangerous in infants and young children, whose livers are still developing and may not fully detoxify ammonia. Conditions like congenital deficiencies in urea cycle enzymes can lead to life-threatening hyperammonemia within days of birth. For example, infants with ornithine transcarbamylase deficiency may present with poor feeding, seizures, and respiratory distress if ammonia levels rise unchecked. Early diagnosis through newborn screening and prompt treatment with medications like sodium benzoate, which binds ammonia for excretion, are crucial in managing these cases.
Practical strategies to mitigate ammonia toxicity include dietary modifications, especially for those with impaired liver function or urea cycle disorders. Reducing protein intake can lower ammonia production, but this must be balanced with adequate nutrition. Supplementation with arginine or citrulline, precursors in the urea cycle, can enhance ammonia conversion to urea. Additionally, medications like lactulose, a non-absorbable disaccharide, reduce ammonia absorption in the gut by acidifying the colon and promoting its excretion. Monitoring ammonia levels through regular blood tests is essential for high-risk individuals to prevent acute toxicity.
In summary, ammonia toxicity is a significant concern due to its detrimental effects on the brain and other organs. The body’s reliance on the urea cycle for detoxification highlights the importance of liver health and adequate nutrient intake. For vulnerable populations, such as infants with genetic disorders or adults with liver disease, proactive management through diet, medication, and monitoring is essential to prevent severe complications. Understanding the mechanisms of ammonia toxicity and its conversion to urea provides a foundation for effective prevention and treatment strategies.
Residential Water Use and Septic Waste: Exploring the Predictive Link
You may want to see also
Explore related products





![]()
Urea Excretion: Role of kidneys in filtering and eliminating urea through urine
Urea, a byproduct of protein metabolism, is a critical waste product that the body must efficiently eliminate to maintain homeostasis. The kidneys play a central role in this process, acting as the primary organs responsible for filtering and excreting urea through urine. This intricate mechanism ensures that excess nitrogen, derived from the breakdown of amino acids, is safely removed from the bloodstream, preventing toxicity. Understanding how the kidneys manage urea excretion is essential for appreciating the body’s metabolic balance and the consequences of renal dysfunction.
The process begins with the filtration of blood in the kidneys’ glomeruli, where urea, along with other waste products and water, is passively filtered into the renal tubules. Unlike substances like glucose, which are actively reabsorbed, urea is not reclaimed by the body. Instead, it continues through the nephron, where water reabsorption in the proximal tubule and loop of Henle concentrates urea in the tubular fluid. This concentration gradient is vital for the kidneys’ ability to produce urine with a higher urea content than the blood, ensuring efficient waste removal. The final step occurs in the collecting ducts, where urea is excreted into the urine, ready for elimination.
From a practical standpoint, maintaining proper kidney function is crucial for effective urea excretion. Dehydration, for instance, can impair this process by reducing blood flow to the kidneys and decreasing urine output, leading to urea buildup. Adults should aim for a daily fluid intake of approximately 2.7 to 3.7 liters (91 to 125 ounces) to support renal function, though individual needs may vary based on activity level, climate, and health status. Additionally, certain medical conditions, such as chronic kidney disease, can disrupt urea excretion, necessitating dietary modifications or medical interventions like dialysis.
Comparatively, the kidneys’ role in urea excretion highlights their superiority over other organs in waste management. While the liver produces urea as part of the urea cycle, it relies entirely on the kidneys for its removal. This interdependence underscores the kidneys’ unique position in systemic waste handling. In contrast, organs like the skin and lungs contribute minimally to urea elimination, emphasizing the kidneys’ irreplaceable function.
In conclusion, the kidneys’ role in filtering and eliminating urea through urine is a testament to their precision and efficiency in maintaining metabolic balance. By understanding this process, individuals can take proactive steps to support kidney health, such as staying hydrated and monitoring protein intake, particularly in older adults or those with pre-existing renal conditions. Recognizing the kidneys’ central role in urea excretion not only highlights their importance but also serves as a reminder of the body’s intricate interdependencies.
Does Your Washing Machine Waste Pipe Need a U-Bend?
You may want to see also
Explore related products






![]()
Protein Metabolism Link: Breakdown of amino acids producing ammonia as a byproduct
Amino acids, the building blocks of proteins, undergo deamination during metabolism, a process that removes an ammonia group (NH₃) from their structure. This ammonia is a toxic byproduct that must be efficiently managed by the body to prevent harm. The liver plays a critical role here, converting ammonia into urea via the urea cycle, a less toxic substance that can be safely excreted in urine. This mechanism highlights the body’s precision in handling metabolic waste, ensuring cellular function while minimizing toxicity.
Consider the implications of excessive protein intake, particularly in individuals with compromised liver function or certain genetic disorders. For instance, a high-protein diet (exceeding 2 grams of protein per kilogram of body weight daily) can overwhelm the liver’s capacity to process ammonia, leading to elevated blood ammonia levels. Symptoms such as nausea, confusion, and fatigue may arise, particularly in those with conditions like hepatic encephalopathy or ornithine transcarbamylase deficiency. Monitoring protein intake and liver health is essential, especially for older adults or those with pre-existing metabolic disorders.
From a practical standpoint, balancing protein consumption with adequate hydration and fiber intake can support the body’s waste management systems. For example, a 70 kg individual should aim for 56–91 grams of protein daily, depending on activity level. Pairing protein-rich meals with water-rich foods (e.g., cucumbers, watermelon) and soluble fiber (e.g., oats, legumes) aids in urea excretion and reduces the risk of ammonia accumulation. Additionally, spacing protein intake evenly throughout the day minimizes metabolic stress on the liver.
Comparatively, the body’s handling of ammonia from protein metabolism contrasts with its management of other waste products, such as carbon dioxide from carbohydrate metabolism. While carbon dioxide is expelled through respiration, ammonia requires complex enzymatic conversion into urea, underscoring the liver’s indispensable role. This distinction emphasizes the need for targeted dietary and lifestyle strategies to support liver health, particularly in populations with increased protein demands, such as athletes or post-surgical patients.
In summary, the breakdown of amino acids during protein metabolism inevitably produces ammonia, a waste product that demands careful regulation. Understanding this process allows for informed dietary choices, particularly for those at risk of metabolic imbalances. By optimizing protein intake, supporting liver function, and adopting practical habits, individuals can mitigate the risks associated with ammonia toxicity and maintain metabolic health.
Does Parking Your Car Waste Gas? Uncovering the Truth Behind Idling
You may want to see also
Explore related products






![]()
Urea Cycle Disorders: Genetic conditions disrupting urea production and causing ammonia buildup
Urea, a metabolic waste product resulting from protein metabolism, is typically eliminated through urine. However, in individuals with urea cycle disorders (UCDs), genetic mutations disrupt this process, leading to a dangerous buildup of ammonia in the bloodstream. These rare but serious conditions highlight the delicate balance required for proper nitrogen disposal in the body.
UCDs stem from defects in one of the six enzymes or transporters involved in the urea cycle, a series of biochemical reactions occurring primarily in the liver. This cycle converts toxic ammonia, a byproduct of protein breakdown, into urea, which is then safely excreted. When any step in this cycle is impaired, ammonia accumulates, causing neurological damage and potentially life-threatening complications.
Recognizing the Signs: A Race Against Time
Infants with severe UCDs often present with symptoms within the first few days of life, including lethargy, poor feeding, vomiting, and seizures. These nonspecific signs can easily be mistaken for other conditions, making prompt diagnosis crucial. Newborn screening programs, now mandatory in many countries, play a vital role in early detection by identifying elevated ammonia levels in blood samples. However, some UCDs may manifest later in childhood or even adulthood, with symptoms triggered by high-protein meals, illness, or stress.
In these cases, individuals may experience headaches, nausea, confusion, and behavioral changes. Without timely intervention, ammonia toxicity can lead to coma, brain damage, and death.
Managing the Disorder: A Lifelong Commitment
Treatment for UCDs focuses on minimizing ammonia production and promoting its removal. This involves a strict low-protein diet, supplemented with essential amino acids and calorie-rich alternatives. Medications like sodium benzoate and sodium phenylbutyrate help bind ammonia for excretion. In severe cases, liver transplantation may be necessary to restore urea cycle function.
Living with UCDs: A Delicate Balance
Individuals with UCDs require lifelong monitoring and management. Regular blood tests to monitor ammonia levels and dietary adjustments are essential. Avoiding high-protein foods, such as meat, dairy, and eggs, is crucial. Close collaboration with a metabolic specialist, dietitian, and other healthcare professionals is vital for optimizing treatment and preventing complications. While UCDs present significant challenges, early diagnosis, proper management, and ongoing research offer hope for improved outcomes and a better quality of life for affected individuals.
Wasteful Society's Hidden Gains: Uncovering Unexpected Benefits in Excess
You may want to see also
Frequently asked questions
Urea is the primary metabolic waste product resulting from protein metabolism.
Urea is produced in the liver through the urea cycle, which involves the breakdown of amino acids, particularly ammonia, a toxic byproduct of protein metabolism.
Urea is considered a waste product because it is a nitrogen-containing compound that the body cannot use and must be excreted, primarily through urine, to prevent toxicity.
If urea is not properly eliminated, it can lead to a condition called uremia, characterized by elevated urea levels in the blood, which can cause symptoms like nausea, fatigue, and in severe cases, kidney failure.