The nephron, the functional unit of the kidney, plays a crucial role in filtering waste from the blood and expelling it from the body. Within the nephron, waste expulsion occurs primarily in the proximal tubule and the loop of Henle through a process called active secretion. Here, substances like hydrogen ions, potassium, and certain drugs are actively transported from the blood into the tubule lumen, joining the waste products already filtered from the glomerulus. As the fluid moves through the distal tubule and collecting duct, water and essential ions are reabsorbed, concentrating the waste into urine. Finally, the waste-laden urine is expelled from the nephron into the ureter and eventually out of the body, completing the process of waste removal.
| Characteristics | Values |
|---|---|
| Location of Waste Expulsion | Primarily occurs in the proximal convoluted tubule (PCT) and loop of Henle. |
| Mechanism | Active transport, passive diffusion, and filtration. |
| Waste Types Expelled | Urea, creatinine, excess ions (e.g., Na⁺, K⁺, Cl⁻), and metabolic byproducts. |
| Role of PCT | Reabsorbs essential nutrients and water while actively secreting waste into the tubule lumen. |
| Role of Loop of Henle | Continues waste concentration through countercurrent multiplication. |
| Role of Distal Tubule | Fine-tunes ion and water balance, further concentrating waste. |
| Final Collection | Waste is collected in the renal pelvis and expelled as urine via the ureter. |
| Energy Requirement | Active transport processes require ATP (e.g., Na⁺/K⁺ ATPase pumps). |
| pH Regulation | Hydrogen ions (H⁺) are secreted into the tubule to maintain blood pH. |
| Hormonal Influence | Aldosterone and ADH regulate ion and water reabsorption, affecting waste concentration. |
Explore related products






What You'll Learn
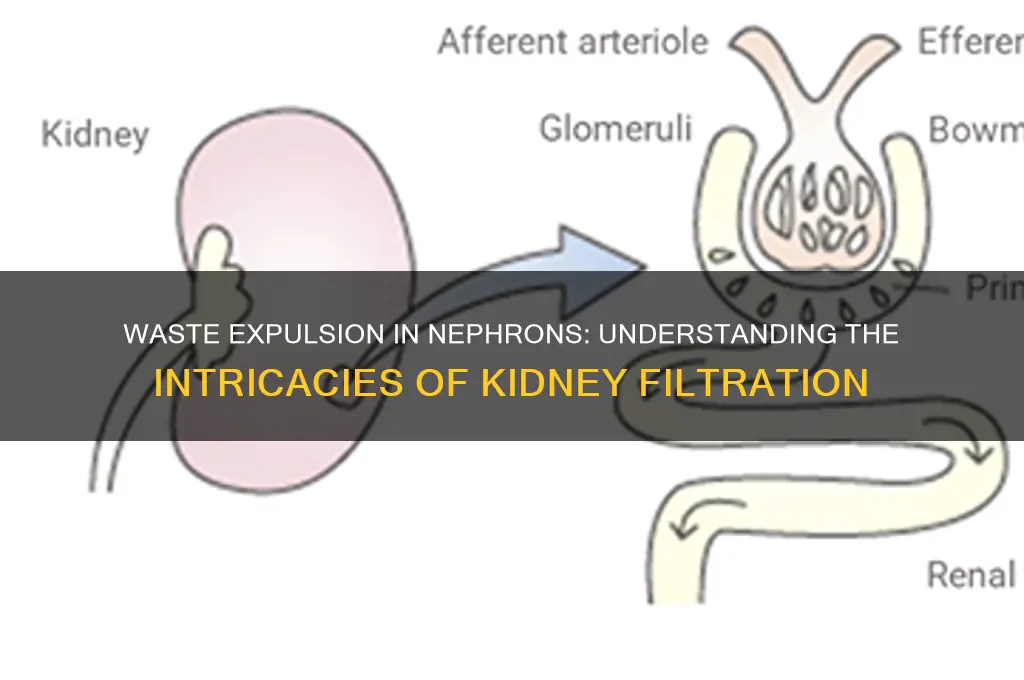
- Filtration at Glomerulus: Waste and excess fluids are filtered from blood into Bowman's capsule
- Reabsorption in PCT: Essential substances like glucose and ions are reabsorbed into the bloodstream
- Secretion in DCT: Hydrogen ions and drugs are actively secreted from blood into the tubule
- Concentration in Loop of Henle: Water reabsorption creates a concentrated waste solution in the tubule
- Excretion in Collecting Duct: Final waste (urine) is transported to the bladder for expulsion
![]()
Filtration at Glomerulus: Waste and excess fluids are filtered from blood into Bowman's capsule
The glomerulus, a dense network of capillaries nestled within the nephron, acts as the kidney's primary filtration unit. Here, a remarkable process unfolds: blood is meticulously sifted, allowing waste products and excess fluids to pass into the surrounding Bowmans capsule while retaining essential cells and proteins. This selective barrier, akin to a finely woven sieve, ensures that only molecules below a certain size threshold, typically around 70 kilodaltons, can traverse into the filtrate.
Consider the mechanics of this filtration. Blood pressure within the glomerular capillaries, approximately 50-60 mmHg, provides the driving force. This hydrostatic pressure pushes water, dissolved solutes, and small molecules like urea, creatinine, and electrolytes through the capillary walls. Simultaneously, the oncotic pressure of plasma proteins, primarily albumin, acts in opposition, pulling fluids back into the bloodstream. The balance between these forces determines the filtration rate, a critical factor in maintaining fluid homeostasis.
A closer examination reveals the glomerular filtration barrier’s intricate structure. It comprises three layers: the endothelial cells of the capillaries, the glomerular basement membrane, and the podocytes with their foot processes. Each layer contributes to the barrier’s selectivity. For instance, the negatively charged glycocalyx on endothelial cells repels negatively charged molecules like albumin, while the basement membrane’s dense matrix further restricts passage. This multi-layered defense ensures that larger proteins and blood cells remain in circulation, preventing their loss in urine.
Practical implications of glomerular filtration extend to clinical scenarios. For example, a decreased filtration rate, as seen in chronic kidney disease, can lead to fluid retention and waste accumulation. Conversely, excessive filtration, often due to hypertension or diabetes, may damage the glomerulus over time. Monitoring glomerular filtration rate (GFR), typically estimated using serum creatinine levels, is a standard diagnostic tool. A GFR below 60 mL/min/1.73 m² for three months indicates kidney dysfunction, necessitating dietary adjustments, medication, or, in severe cases, dialysis.
In summary, filtration at the glomerulus is a precise, pressure-driven process that separates waste and excess fluids from the bloodstream. Its efficiency relies on a sophisticated barrier system and the balance of hydrostatic and oncotic pressures. Understanding this mechanism not only highlights the kidney’s role in waste expulsion but also underscores the importance of maintaining glomerular health for overall well-being.
How the USA Squandered Billions in Double Payments: A Costly Oversight
You may want to see also
Explore related products






![]()
Reabsorption in PCT: Essential substances like glucose and ions are reabsorbed into the bloodstream
The proximal convoluted tubule (PCT) is a powerhouse of reabsorption, reclaiming essential substances from the filtrate before they're lost in urine. Imagine a meticulous gatekeeper, selectively allowing vital molecules like glucose, amino acids, and electrolytes (sodium, chloride, bicarbonate) to re-enter the bloodstream while waste products continue their journey towards excretion. This process, driven by active transport and facilitated diffusion, ensures our bodies retain what they need while efficiently eliminating what they don't.
Glucose, for instance, is reabsorbed against its concentration gradient through a sodium-glucose cotransporter (SGLT2), highlighting the energy-dependent nature of this process.
Understanding the mechanisms behind PCT reabsorption is crucial for appreciating the nephron's role in maintaining homeostasis. Think of it as a finely tuned recycling system. Sodium, the most abundant cation in extracellular fluid, is actively pumped out of the PCT cells into the interstitium, creating an electrochemical gradient that pulls other substances, like chloride and water, along with it. This process, known as coupled transport, demonstrates the nephron's ability to leverage one process to drive another, maximizing efficiency.
Bicarbonate, essential for maintaining blood pH, is reabsorbed through a complex mechanism involving carbonic anhydrase and a chloride-bicarbonate exchanger. This intricate dance ensures our blood remains slightly alkaline, a critical factor for enzymatic function and overall health.
The PCT's reabsorptive capacity is not limitless. Conditions like diabetes mellitus can overwhelm the SGLT2 transporters, leading to glucosuria, where glucose spills into the urine. This highlights the delicate balance between reabsorption and filtration, and how disruptions can have significant health consequences. Similarly, mutations in chloride channel genes can lead to conditions like Bartter syndrome, characterized by excessive salt and water loss.
Optimizing PCT function is key to overall kidney health. Staying hydrated ensures adequate blood flow to the nephrons, facilitating efficient filtration and reabsorption. A balanced diet rich in fruits and vegetables provides essential electrolytes and supports the intricate transport mechanisms within the PCT. While certain medications can impact reabsorption, always consult a healthcare professional before making any changes to your medication regimen. By understanding the PCT's role in reabsorption, we gain a deeper appreciation for the nephron's remarkable ability to maintain the body's delicate internal balance.
Yumi's Smart Strategies to Prevent Smoothie Waste and Maximize Freshness
You may want to see also
Explore related products






![]()
Secretion in DCT: Hydrogen ions and drugs are actively secreted from blood into the tubule
The distal convoluted tubule (DCT) plays a critical role in waste expulsion within the nephron by actively secreting hydrogen ions (H⁺) and certain drugs from the blood into the tubule lumen. This process is essential for maintaining acid-base balance and eliminating foreign substances from the body. Unlike passive filtration in the glomerulus, secretion in the DCT is energy-dependent, relying on transport proteins like the H⁺-ATPase pump. This mechanism ensures that excess H⁺ ions, which can disrupt systemic pH, are efficiently removed. Similarly, drugs such as penicillin and lithium are secreted here, preventing their accumulation and potential toxicity. Understanding this process highlights the DCT’s dual function in both homeostasis and detoxification.
Analyzing the secretion of hydrogen ions in the DCT reveals its significance in acid-base regulation. When blood pH drops (acidosis), the DCT increases H⁺ secretion to restore balance. This is achieved through the H⁺-ATPase pump, which actively transports H⁺ ions against their concentration gradient. For instance, in diabetic ketoacidosis, where blood pH can fall below 7.3, the DCT works overtime to expel excess H⁺ ions. Clinically, this process can be modulated by medications like acetazolamide, which inhibits carbonic anhydrase and indirectly enhances H⁺ secretion. However, overactivity of this mechanism can lead to metabolic alkalosis, underscoring the need for precise regulation.
The secretion of drugs in the DCT is a vital yet often overlooked aspect of renal function. Many drugs, including penicillin and methotrexate, are actively transported into the tubule lumen via organic anion transporters (OATs). This process reduces their systemic concentration, preventing toxicity. For example, in patients on high-dose penicillin therapy (up to 20 million units/day), the DCT ensures rapid elimination, minimizing the risk of adverse effects. However, this mechanism can also lead to drug-drug interactions; nonsteroidal anti-inflammatory drugs (NSAIDs) compete with OATs, potentially increasing the toxicity of concurrently administered medications. Healthcare providers must consider these interactions when prescribing drugs excreted via the DCT.
Practical considerations for optimizing DCT secretion include monitoring renal function and adjusting dosages accordingly. In patients with reduced glomerular filtration rate (GFR), drug accumulation is more likely, necessitating lower doses. For instance, lithium, a drug primarily excreted by the DCT, requires dose reductions in elderly patients or those with chronic kidney disease (CKD). Hydration status also impacts secretion efficiency; dehydration reduces blood flow to the kidneys, impairing DCT function. Encouraging adequate fluid intake (2–3 liters/day for adults) can enhance waste expulsion. Finally, avoiding concurrent use of drugs that compete for DCT transporters can prevent unintended toxicity.
In conclusion, secretion in the DCT is a specialized process that safeguards systemic homeostasis by expelling hydrogen ions and drugs. Its energy-dependent mechanisms, while efficient, require careful management to avoid complications. Clinicians and patients alike must recognize the DCT’s role in drug elimination, particularly for medications like penicillin and lithium. By understanding this process, healthcare providers can optimize therapy, minimize adverse effects, and ensure effective waste expulsion within the nephron. This knowledge underscores the importance of the DCT in both renal physiology and clinical practice.
Warm Wastewater's Impact: Accelerating Algae Growth in Aquatic Ecosystems
You may want to see also
Explore related products






![]()
Concentration in Loop of Henle: Water reabsorption creates a concentrated waste solution in the tubule
The Loop of Henle, a U-shaped segment of the nephron, is a marvel of efficiency in waste concentration. Here, a countercurrent multiplier system operates, allowing for the creation of a hypertonic environment in the renal medulla. This process is crucial for the kidney's ability to conserve water and concentrate waste products before they are expelled. As fluid flows through the descending limb of the Loop of Henle, water is passively reabsorbed into the surrounding interstitium due to the increasing osmotic gradient. This reabsorption is driven by the presence of urea and sodium chloride, which accumulate in the medulla, creating a highly concentrated environment.
Consider the mechanism in action: as water leaves the descending limb, the remaining fluid becomes progressively more concentrated. By the time it reaches the ascending limb, the solution is significantly hypertonic. This concentration gradient is essential for the kidney's function, enabling it to produce urine that is much more concentrated than the body's intracellular fluid. For instance, in a healthy adult, the Loop of Henle can generate a medullary interstitium with an osmolarity of up to 1200 mOsm/L, compared to the plasma osmolarity of approximately 290 mOsm/L. This stark difference highlights the efficiency of the countercurrent system.
To understand the practical implications, imagine a scenario where water conservation is critical, such as in dehydration. The Loop of Henle's ability to concentrate waste becomes a survival mechanism. By maximizing water reabsorption, the body can produce highly concentrated urine, minimizing fluid loss. However, this process is not without its limitations. In individuals with impaired kidney function, such as those with chronic kidney disease, the concentration mechanism may fail, leading to the production of large volumes of dilute urine, a condition known as polyuria.
A key takeaway is the importance of maintaining a healthy osmotic balance. For optimal kidney function, it is essential to stay well-hydrated, especially in hot climates or during physical exertion. Practical tips include monitoring urine color, which should be pale yellow, and ensuring adequate fluid intake, typically around 2-3 liters per day for adults. Additionally, reducing salt intake can alleviate the workload on the kidneys, as excessive sodium increases the osmotic load, potentially disrupting the delicate balance in the Loop of Henle.
In summary, the concentration of waste in the Loop of Henle is a sophisticated process that relies on water reabsorption and a countercurrent multiplier system. This mechanism not only conserves water but also ensures that waste products are efficiently expelled in a concentrated form. By understanding this process, individuals can take proactive steps to support kidney health, such as maintaining proper hydration and moderating salt intake. This knowledge is particularly valuable for those at risk of kidney-related issues, emphasizing the importance of preventive measures in maintaining overall well-being.
Sewage Waste Disposal: Methods for Managing and Eliminating Sold Byproducts
You may want to see also
Explore related products






![]()
Excretion in Collecting Duct: Final waste (urine) is transported to the bladder for expulsion
The collecting duct serves as the final gateway for waste expulsion in the nephron, a critical process that ensures the body’s internal environment remains balanced. After filtration, reabsorption, and secretion in earlier nephron segments, the final waste product, urine, is funneled into the collecting duct. Here, the urine undergoes fine-tuning adjustments in concentration and volume, primarily through the regulation of water and solute transport. This process is tightly controlled by hormones like antidiuretic hormone (ADH), which acts on aquaporin channels to either retain or release water, depending on the body’s hydration status. Without this precise regulation, urine would either be too dilute or too concentrated, disrupting fluid and electrolyte balance.
Consider the journey of urine through the collecting duct as a final quality check before expulsion. Once the urine leaves the collecting duct, it enters the renal pelvis and then the ureter, a muscular tube that propels it toward the bladder via peristaltic waves. This transport mechanism is passive yet efficient, relying on the ureter’s rhythmic contractions to move urine without requiring conscious effort. For optimal function, staying hydrated is key; adequate water intake ensures urine flows smoothly through the ureter, reducing the risk of stasis and potential infections. Adults should aim for 2–3 liters of water daily, though individual needs vary based on activity level, climate, and health conditions.
A critical aspect of this phase is the bladder’s role as a temporary storage reservoir. The bladder’s elastic walls expand to accommodate urine, holding up to 500 milliliters in adults before signaling the need for expulsion. This storage capacity is vital for daily convenience, but it also poses risks if urine remains in the bladder for too long. Prolonged retention can lead to bacterial growth, increasing the likelihood of urinary tract infections (UTIs). Practical tips include avoiding holding urine for extended periods and practicing good hygiene, such as wiping front to back to prevent bacterial transfer. For those with urinary incontinence or frequent UTIs, consulting a healthcare provider for tailored management strategies is essential.
Comparatively, the collecting duct’s role in waste expulsion highlights the nephron’s efficiency as a microcosm of the body’s waste management system. While earlier segments focus on filtration and reabsorption, the collecting duct and subsequent structures prioritize safe and controlled removal. This division of labor ensures that waste is not only processed but also expelled in a manner that minimizes risk to the body. Understanding this process underscores the importance of maintaining kidney health through lifestyle choices, such as a balanced diet, regular exercise, and avoiding nephrotoxic substances like excessive NSAIDs or alcohol. By appreciating the collecting duct’s function, individuals can take proactive steps to support their kidneys and, by extension, their overall well-being.
Waste Motor Oil Burning Temperatures: Understanding the Heat Intensity
You may want to see also
Frequently asked questions
Waste is expelled through the process of filtration, reabsorption, and secretion within the nephron. Blood is filtered in the glomerulus, waste products like urea and excess ions are retained in the tubule, and water and essential substances are reabsorbed, while remaining waste is concentrated and expelled as urine.
The glomerulus filters waste from the blood, the proximal tubule reabsorbs essential substances while retaining waste, the loop of Henle concentrates waste, and the distal tubule and collecting duct fine-tune waste concentration before expulsion through the ureter.
The nephron selectively reabsorbs essential substances like glucose, amino acids, and electrolytes in the proximal tubule, while waste products like urea and excess ions are not reabsorbed, allowing them to be concentrated and expelled as urine.