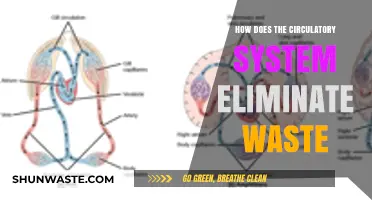
The human body continuously produces nitrogenous waste, primarily in the form of urea, as a byproduct of protein metabolism and the breakdown of amino acids. This waste is toxic and must be efficiently eliminated to maintain homeostasis. The process begins in the liver, where ammonia, a highly toxic nitrogenous waste, is converted into urea through the urea cycle. Urea is then transported via the bloodstream to the kidneys, which filter it out of the blood and into the urine. Finally, the urinary system expels the urea-laden urine from the body, ensuring the safe removal of nitrogenous waste and preventing its accumulation, which could otherwise lead to severe health complications.
Explore related products






What You'll Learn
- Urea Formation in Liver: Ammonia converted to urea via ornithine cycle, reducing toxicity for safe excretion
- Kidney Filtration: Glomeruli filter blood, removing urea and waste into urine
- Tubular Reabsorption: Proximal tubules reclaim essential nutrients, leaving waste for elimination
- Urine Concentration: Loop of Henle adjusts water reabsorption, concentrating waste in urine
- Bladder Storage & Excretion: Urine stored in bladder, expelled via urethra, removing nitrogenous waste
![]()
Urea Formation in Liver: Ammonia converted to urea via ornithine cycle, reducing toxicity for safe excretion
Ammonia, a byproduct of protein metabolism, is highly toxic to the brain and other tissues. To neutralize this threat, the liver orchestrates a complex biochemical process known as the ornithine cycle, converting ammonia into urea—a far less harmful compound. This cycle is a metabolic marvel, involving a series of enzymatic reactions that not only detoxify ammonia but also prepare it for safe elimination through urine.
The ornithine cycle begins with the combination of ammonia and carbon dioxide to form carbamoyl phosphate, catalyzed by the enzyme carbamoyl phosphate synthetase I. This step is crucial, as it traps ammonia in a less toxic form. Next, ornithine, an amino acid, reacts with carbamoyl phosphate to produce citrulline, facilitated by ornithine transcarbamylase. Citrulline then travels from the mitochondria to the cytosol, where it combines with another ammonia molecule and aspartate to form argininosuccinate, under the action of argininosuccinate synthetase. Finally, argininosuccinate lyase cleaves argininosuccinate into fumarate and arginine. Arginine is hydrolyzed by arginase to release urea and regenerate ornithine, completing the cycle.
While the ornithine cycle is efficient, certain conditions can disrupt its function. For instance, liver disease or genetic defects in cycle enzymes can lead to hyperammonemia, a dangerous buildup of ammonia in the blood. Infants with inborn errors of urea cycle metabolism, such as ornithine transcarbamylase deficiency, may require immediate medical intervention, including protein-restricted diets and medications like sodium benzoate or phenylbutyrate to help eliminate excess nitrogen. Adults with liver failure may need dialysis or liver transplantation to manage ammonia toxicity.
Practical tips for supporting urea formation include maintaining a balanced diet to avoid excessive protein intake, especially in individuals with compromised liver function. Staying hydrated is also essential, as adequate water intake promotes the excretion of urea through urine. For those at risk of hyperammonemia, regular monitoring of ammonia levels and adherence to prescribed treatments are critical. Understanding the ornithine cycle highlights the liver’s role as a metabolic powerhouse, transforming a toxic waste product into a manageable compound for safe elimination.
Understanding the Journey: Liquid Waste Through the Urinary System
You may want to see also
Explore related products





![]()
Kidney Filtration: Glomeruli filter blood, removing urea and waste into urine
The kidneys are the body's primary filtration system, and at the heart of this process are the glomeruli, tiny, dense networks of capillaries that act as the first line of defense against nitrogenous waste. These microscopic structures are so efficient that they filter approximately 125 milliliters of blood per minute, or about 180 liters per day, in a healthy adult. This filtration process is crucial for removing urea, a byproduct of protein metabolism, and other waste products from the bloodstream, ensuring they are excreted in urine rather than accumulating to toxic levels.
Consider the glomeruli as the bouncers of a highly exclusive club, allowing only certain substances to pass through while ejecting unwanted guests. In this case, the "club" is the bloodstream, and the "unwanted guests" are waste products like urea, creatinine, and excess ions. The glomerular filtration barrier, composed of endothelial cells, a basement membrane, and epithelial cells (podocytes), selectively permits small molecules such as water, electrolytes, and waste to pass into the nephron, the functional unit of the kidney. Larger molecules like proteins and blood cells are retained in the circulation, maintaining the integrity of the blood while effectively clearing waste.
To optimize kidney filtration and support glomerular function, certain practical steps can be taken. Staying adequately hydrated is paramount, as it helps maintain blood volume and flow rate through the kidneys, facilitating efficient filtration. Aim for 2–3 liters of water daily, adjusting for activity level, climate, and health conditions. Additionally, moderating protein intake can reduce the burden on the kidneys, as excessive protein consumption increases urea production. For adults, the recommended dietary allowance (RDA) for protein is 0.8 grams per kilogram of body weight, though this may vary based on age, sex, and activity level.
A comparative analysis highlights the glomeruli's role in contrast to other waste elimination systems. While the liver processes ammonia into urea through the urea cycle, the kidneys take over the final step of excretion. Unlike the lungs, which eliminate gaseous waste like carbon dioxide, or the skin, which excretes small amounts of urea and salts through sweat, the kidneys handle the bulk of nitrogenous waste. This specialization underscores the glomeruli's critical function in maintaining homeostasis, as even a 50% reduction in glomerular filtration rate (GFR) can indicate significant kidney impairment, necessitating medical intervention.
In conclusion, the glomeruli's role in kidney filtration is both precise and indispensable. By understanding their function and adopting supportive habits, individuals can safeguard their renal health and ensure the efficient elimination of nitrogenous waste. Regular monitoring of kidney function, especially for those at risk of chronic kidney disease (e.g., diabetics, hypertensives, or individuals over 60), is essential. Early detection of reduced GFR or abnormalities in urine composition can lead to timely interventions, preserving kidney function and overall well-being.
Smoking Cigarettes: A Costly Habit Draining Your Finances and Health
You may want to see also
Explore related products






![]()
Tubular Reabsorption: Proximal tubules reclaim essential nutrients, leaving waste for elimination
The kidneys are the unsung heroes of waste management in the body, and their intricate processes ensure that harmful substances are eliminated while vital nutrients are retained. One crucial step in this delicate balance is tubular reabsorption, a process that occurs primarily in the proximal tubules of the nephron. These tiny, highly specialized structures act as gatekeepers, selectively reclaiming essential molecules from the filtrate produced by the glomerulus.
Imagine a sophisticated recycling center where valuable resources are recovered from a waste stream. The proximal tubules perform a similar function, reabsorbing approximately 65-70% of the filtered sodium, water, and other key solutes, including glucose, amino acids, and bicarbonate. This reabsorption is driven by active transport mechanisms, such as sodium-glucose cotransporters (SGLTs) and sodium-bicarbonate cotransporters, which ensure that these essential nutrients are returned to the bloodstream. For instance, SGLT2 in the proximal tubule is responsible for reabsorbing up to 90% of filtered glucose, a process that can be inhibited by medications like empagliflozin to treat diabetes and heart failure.
While the proximal tubules are busy reclaiming what the body needs, they also play a critical role in leaving behind what it doesn’t. Nitrogenous waste, such as urea and creatinine, is largely excluded from this reabsorption process. These waste products, derived from the breakdown of proteins and nucleic acids, are allowed to continue their journey through the nephron, eventually reaching the bladder for excretion in urine. This selective process ensures that the body maintains homeostasis, preventing the accumulation of toxic byproducts while conserving essential nutrients.
Understanding tubular reabsorption is not just an academic exercise; it has practical implications for health and disease. For example, conditions like proximal tubular dysfunction, often seen in chronic kidney disease or acute kidney injury, can impair the reabsorption of critical substances like bicarbonate, leading to metabolic acidosis. Conversely, excessive reabsorption of sodium and water in the proximal tubule can contribute to hypertension. Clinicians often target these pathways with medications, such as diuretics or SGLT2 inhibitors, to manage fluid balance and electrolyte levels in patients.
In essence, the proximal tubules are the body’s meticulous sorters, distinguishing between what is valuable and what is waste. By reclaiming essential nutrients while allowing nitrogenous waste to pass through, they ensure that the body remains a well-oiled machine, free from the burden of harmful byproducts. This process underscores the elegance of renal physiology and highlights the importance of maintaining kidney health for overall well-being.
Human Impact on Mass Wasting: Causes, Consequences, and Prevention
You may want to see also
Explore related products






![]()
Urine Concentration: Loop of Henle adjusts water reabsorption, concentrating waste in urine
The human body is a marvel of efficiency, especially when it comes to waste management. One of the most critical processes is the elimination of nitrogenous waste, primarily in the form of urea, which is a byproduct of protein metabolism. The kidneys play a central role in this process, and within them, the Loop of Henle is a key structure that fine-tunes urine concentration by adjusting water reabsorption. This mechanism ensures that waste is efficiently concentrated in urine while maintaining the body’s fluid balance.
Consider the Loop of Henle as a sophisticated filtration system. It consists of a descending limb, a thin segment, an ascending limb, and a thick segment, each with distinct functions. In the descending limb, water is passively reabsorbed into the bloodstream, driven by the osmotic gradient created by sodium and chloride ions. This process dilutes the blood but concentrates the urine in the renal tubule. Conversely, the ascending limb actively pumps sodium and chloride ions out of the tubule and into the surrounding interstitium, creating a hypertonic environment that prevents water reabsorption. This countercurrent mechanism allows for precise control over urine concentration, ensuring that waste products like urea are effectively retained in the urine while water is conserved.
For example, in a dehydrated state, the body activates antidiuretic hormone (ADH), which enhances water reabsorption in the descending limb and increases the osmotic gradient in the medulla of the kidney. This results in the production of highly concentrated urine, minimizing water loss while still eliminating waste. Conversely, in a hydrated state, ADH secretion decreases, reducing water reabsorption and producing dilute urine to expel excess water. This dynamic adjustment is essential for survival in varying environmental conditions, from arid deserts to humid climates.
Practical implications of this process are significant, especially for individuals with kidney disorders or those in extreme environments. For instance, patients with chronic kidney disease often struggle with urine concentration, leading to frequent urination and dehydration. Understanding the Loop of Henle’s role can guide treatments such as fluid management and medication like diuretics or ADH analogs. Athletes or hikers in water-scarce regions can benefit from knowing how hydration levels affect urine concentration, ensuring they conserve water without compromising waste elimination.
In conclusion, the Loop of Henle is not just a structural component of the kidney but a master regulator of urine concentration. Its ability to adjust water reabsorption based on the body’s needs ensures that nitrogenous waste is efficiently eliminated while maintaining fluid balance. By appreciating this mechanism, we can better address health challenges and optimize physiological performance in diverse conditions. Whether in a clinical setting or the great outdoors, understanding this process empowers us to make informed decisions about hydration and waste management.
How Rabbits Efficiently Eliminate Waste: A Natural Process Explained
You may want to see also
Explore related products






![]()
Bladder Storage & Excretion: Urine stored in bladder, expelled via urethra, removing nitrogenous waste
The bladder, a hollow organ in the pelvis, serves as a reservoir for urine, the body's liquid waste product. This storage function is critical for maintaining homeostasis, allowing individuals to control the timing of waste elimination rather than expelling it continuously. Urine, primarily composed of water, electrolytes, and waste products like urea, is produced by the kidneys as they filter blood. Urea, a nitrogenous waste, is the end product of protein metabolism and must be efficiently removed to prevent toxicity. Once formed, urine travels from the kidneys through the ureters into the bladder, where it is stored until expulsion.
The process of expelling urine, known as micturition, involves a coordinated effort between the bladder, urethra, and nervous system. As the bladder fills, stretch receptors in its walls signal the brain, creating the urge to urinate. When ready, the detrusor muscle in the bladder wall contracts, while the urethral sphincter relaxes, allowing urine to flow out of the body via the urethra. This mechanism ensures the removal of nitrogenous waste, primarily urea, along with other toxins and excess substances. For adults, a healthy bladder can hold approximately 400–600 milliliters of urine, though the urge to urinate typically occurs when the bladder is about one-third full.
Proper bladder function is essential for overall health, particularly in eliminating nitrogenous waste. Conditions like urinary incontinence, urinary tract infections, or bladder stones can disrupt this process, leading to waste retention and potential toxicity. For instance, urea buildup in the blood, a condition called azotemia, can occur if urine is not expelled efficiently. Practical tips to support bladder health include staying hydrated (aiming for 1.5–2 liters of water daily), avoiding excessive caffeine or alcohol, and practicing pelvic floor exercises, especially for older adults or postpartum individuals.
Comparatively, the bladder’s role in waste elimination is distinct from other excretory systems, such as sweating or breathing, which handle different types of waste. While the skin eliminates salts and small amounts of urea through sweat, and the lungs expel carbon dioxide, the bladder is the primary route for removing urea and other nitrogenous byproducts. This specialization underscores the bladder’s unique importance in maintaining nitrogen balance in the body. For children, bladder training techniques, such as scheduled bathroom breaks and positive reinforcement, can help establish healthy urinary habits early on.
In conclusion, the bladder’s storage and excretion function is a vital component of the body’s waste management system, specifically targeting nitrogenous waste like urea. Understanding this process highlights the importance of maintaining bladder health through hydration, lifestyle adjustments, and proactive care. By ensuring efficient urine expulsion, individuals can prevent waste accumulation and support overall metabolic health. Whether for children, adults, or the elderly, prioritizing bladder function is key to a well-functioning excretory system.
Holiday Waste's Environmental Impact: Unwrapping the Hidden Costs of Celebrations
You may want to see also
Frequently asked questions
Nitrogenous wastes are byproducts of protein metabolism, primarily urea, uric acid, and ammonia. They are toxic in high concentrations and must be eliminated to prevent damage to tissues and organs, maintain pH balance, and ensure overall health.
The body breaks down proteins into amino acids through digestion. Excess amino acids are deaminated in the liver, where the nitrogen is converted into ammonia. Ammonia is then converted to urea in the urea cycle, a less toxic compound that can be safely excreted.
The liver processes ammonia into urea, which is then transported to the kidneys via the bloodstream. The kidneys filter urea from the blood and excrete it in urine. Additionally, a small amount of nitrogenous waste is eliminated through sweat and exhaled air as ammonia.