The question of whether unused morphine needs to be wasted is a critical issue in healthcare settings, particularly in pain management and end-of-life care. Morphine, a potent opioid, is often administered in controlled doses, but circumstances such as patient refusal, changes in treatment plans, or medication errors can result in unused portions. Healthcare providers must adhere to strict protocols to ensure patient safety and regulatory compliance, which often dictate that unused medications, including morphine, be discarded or wasted to prevent diversion, misuse, or accidental administration. However, this practice raises concerns about medication waste, cost implications, and the ethical use of resources. Balancing these considerations requires a thorough understanding of institutional policies, legal requirements, and the potential risks associated with retaining unused morphine.
| Characteristics | Values |
|---|---|
| Requirement to Waste Unused Morphine | Depends on institutional policies, state regulations, and DEA guidelines. Generally, controlled substances like morphine must be wasted if not administered to the patient. |
| Reason for Wasting | To prevent diversion, misuse, or theft of controlled substances. |
| Documentation | Wasting must be documented, including the amount, method of waste, and witnesses (if required). |
| Witness Requirement | Often requires a second healthcare professional to witness the wasting process, especially in hospital settings. |
| Storage of Unused Morphine | Cannot be stored for later use due to regulatory restrictions on controlled substances. |
| Exceptions | Some facilities may allow return to pharmacy under specific conditions, but this is rare and depends on local regulations. |
| DEA Guidelines | Unused controlled substances must be disposed of in accordance with DEA regulations (e.g., 21 CFR 1307.21). |
| State Regulations | Varies by state; some states have stricter requirements than federal guidelines. |
| Environmental Disposal | Must follow local, state, and federal guidelines for disposal of controlled substances (e.g., DEA-approved methods). |
| Training | Staff must be trained on proper wasting procedures to ensure compliance with regulations. |
Explore related products






What You'll Learn
- Proper Disposal Methods: Safe and compliant ways to dispose of unused morphine to prevent misuse
- Legal Requirements: Regulations and laws governing the disposal of controlled substances like morphine
- Documentation Practices: Accurate recording of wasted morphine to maintain accountability and compliance
- Storage Guidelines: Proper storage of unused morphine to ensure safety and prevent diversion
- Witness Protocols: Requirement for a witness during the wasting process to ensure transparency
![]()
Proper Disposal Methods: Safe and compliant ways to dispose of unused morphine to prevent misuse
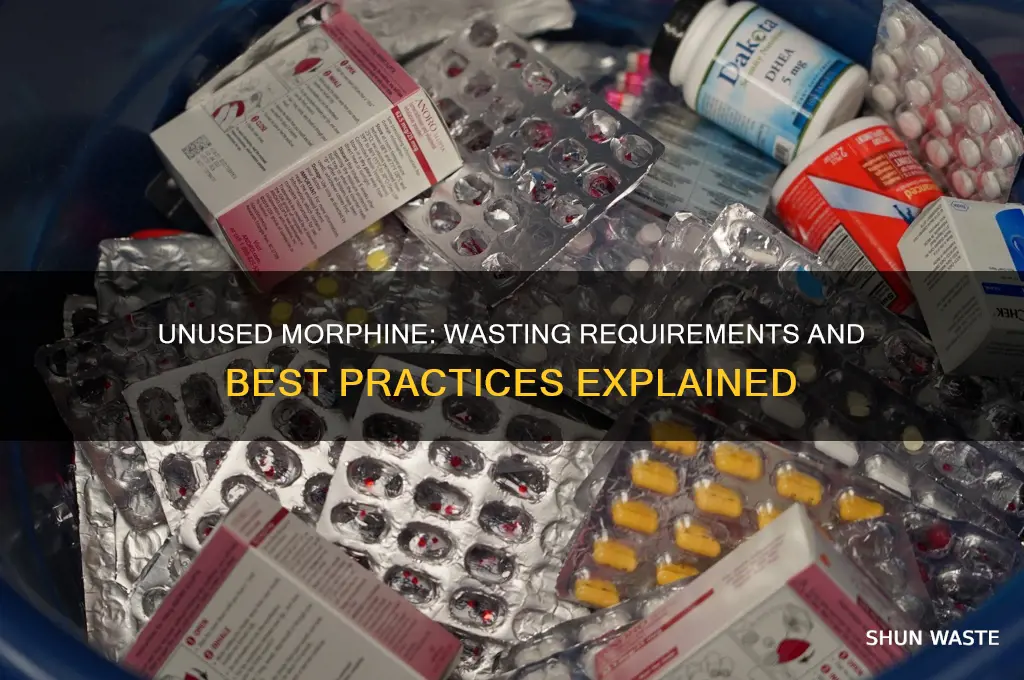
Unused morphine poses a significant risk if left unsecured, as it can be diverted for misuse, leading to addiction, overdose, or death. Proper disposal is not just a recommendation—it’s a critical responsibility for anyone handling this potent opioid. The DEA and FDA emphasize that flushing morphine down the toilet is no longer the default method due to environmental concerns, though it remains an option for specific formulations listed on the FDA’s flush list, such as immediate-release tablets or liquid morphine in concentrations over 100 mg/mL. For all other forms, including extended-release tablets and lower-concentration liquids, safer alternatives must be prioritized.
One widely endorsed method is drug take-back programs, which provide secure disposal through authorized pharmacies, hospitals, or law enforcement agencies. These programs ensure morphine is incinerated at high temperatures, rendering it inactive. To locate a nearby take-back site, use the DEA’s collection site locator or inquire at local pharmacies. If immediate disposal is necessary and no take-back option is available, morphine can be mixed with an unpalatable substance like dirt, cat litter, or coffee grounds in a sealed plastic bag before tossing into household trash. This method deters accidental ingestion or intentional retrieval but does not neutralize the drug’s potency.
For healthcare facilities, compliance with DEA regulations is non-negotiable. Unused morphine must be documented, witnessed, and disposed of according to state and federal guidelines. This often involves returning controlled substances to a reverse distributor or using on-site waste systems approved for pharmaceutical destruction. Home users should never return unused morphine to pharmacies or share it with others, as this violates legal and safety protocols. Instead, they should follow FDA guidelines for at-home disposal, ensuring the medication is unrecoverable before discarding.
A comparative analysis reveals that while flushing remains the fastest method for high-risk formulations, take-back programs offer the most environmentally and socially responsible solution. Mixing with undesirable substances serves as a practical stopgap but should not replace permanent disposal. Each method has its limitations: flushing contributes to water contamination, take-back programs require accessibility, and at-home deactivation is less foolproof. The choice depends on the morphine formulation, local resources, and urgency, but the goal remains consistent—preventing diversion and harm.
In conclusion, proper disposal of unused morphine is a multifaceted issue requiring awareness, accessibility, and action. Whether through take-back programs, approved at-home methods, or regulated institutional procedures, the priority is to eliminate the risk of misuse while minimizing environmental impact. By adhering to these guidelines, individuals and institutions can fulfill their ethical and legal obligations, safeguarding both public health and the planet.
How the Lymphatic System Filters Metabolic Waste: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Legal Requirements: Regulations and laws governing the disposal of controlled substances like morphine
The disposal of controlled substances, including morphine, is tightly regulated to prevent misuse, diversion, and environmental harm. In the United States, the Drug Enforcement Administration (DEA) enforces the Controlled Substances Act (CSA), which classifies morphine as a Schedule II drug due to its high potential for abuse and severe dependence liability. Under these regulations, unused morphine must be disposed of in compliance with specific legal requirements, which vary depending on whether the disposal is occurring in a healthcare setting, pharmacy, or at home.
For healthcare facilities, the DEA mandates that unused morphine be "wasted" in the presence of a witness, typically another healthcare professional. This process involves documenting the amount of unused medication, the reason for wastage, and the names of the individuals involved. The DEA’s 21 CFR Part 1301.22 outlines that controlled substances must be destroyed in a manner that renders them non-retrievable, such as by incineration or through a DEA-registered reverse distributor. Failure to adhere to these regulations can result in severe penalties, including fines and loss of licensure.
At the state level, additional laws may impose stricter requirements. For example, some states require healthcare providers to use DEA-approved waste vendors or to follow specific protocols for witness verification. In California, the Board of Pharmacy mandates that controlled substances be disposed of within 72 hours of being deemed waste, with detailed records maintained for at least three years. These state-specific regulations often complement federal laws, creating a layered compliance framework that providers must navigate carefully.
For patients or caregivers disposing of unused morphine at home, the DEA and the Food and Drug Administration (FDA) provide guidelines under the Secure and Responsible Drug Disposal Act. This act allows for the use of drug take-back programs, which are preferred over flushing medications down the toilet due to environmental concerns. If a take-back program is unavailable, the FDA recommends mixing the morphine with an unpalatable substance (e.g., dirt, cat litter) in a sealed container before disposal in the trash. However, this method is not permitted for Schedule II drugs like morphine in all states, emphasizing the need to check local regulations.
In summary, the legal requirements for disposing of unused morphine are stringent and multifaceted, reflecting the drug’s classification as a controlled substance. Healthcare providers, pharmacies, and individuals must adhere to federal and state regulations to ensure compliance, avoid penalties, and protect public health. Practical steps include verifying witness protocols, using approved disposal methods, and staying informed about jurisdictional variations in the law.
Handling Composite Waste Particles: Effective Management and Disposal Methods
You may want to see also
Explore related products






![]()
Documentation Practices: Accurate recording of wasted morphine to maintain accountability and compliance
Unused morphine, whether in liquid or tablet form, must be documented as wasted to ensure accountability and compliance with regulatory standards. This process is not merely bureaucratic; it directly impacts patient safety, legal liability, and institutional trust. For instance, a 10 mg/mL morphine solution drawn into a syringe but not administered requires immediate documentation of the wasted amount, including the witness signature if facility policy mandates it. Failure to record such instances can lead to discrepancies in controlled substance logs, triggering audits or investigations.
Accurate documentation begins with clarity in recording methods. Use standardized forms or electronic health records (EHRs) to log the morphine concentration (e.g., 2 mg/mL), volume drawn (e.g., 5 mL), and total wasted dose (10 mg in this case). Include timestamps and the reason for wastage, such as "patient refused" or "medication expired." For pediatric doses, specify the age-based calculation (e.g., 0.1 mg/kg for a 10 kg child) and the corresponding wasted amount if the dose was prepared but not given. Inconsistencies, such as rounding errors or omitted details, can undermine audit trails and raise suspicion of diversion.
Witnessed wastage is a critical safeguard, particularly for high-risk medications like morphine. If a colleague observes the disposal, their signature on the documentation adds a layer of verification. For example, a nurse preparing 15 mg of morphine sulfate for post-surgical pain relief but discarding 5 mg due to a spill should have another licensed professional confirm the process. Institutions should train staff to prioritize this step, even in time-sensitive scenarios, as it mitigates risks of misuse or theft.
Electronic systems streamline documentation but require vigilance to avoid errors. Auto-population fields in EHRs can mistakenly carry forward incorrect data, such as a wasted dose from a previous shift. Always cross-verify entries, especially when dealing with partial doses (e.g., 2.5 mg wasted from a 10 mg preparation). Regularly audit logs to identify patterns, such as frequent wastage by a specific staff member or during particular shifts, which may indicate training gaps or systemic issues.
Ultimately, meticulous documentation of wasted morphine is non-negotiable. It protects patients by ensuring medication availability, safeguards providers from allegations of misconduct, and upholds institutional integrity. Treat each entry as a legal record, not a routine task. By embedding precision and transparency into this practice, healthcare teams fortify their commitment to ethical care and regulatory adherence.
Industrial Waste and Surface Waters: Environmental Impact and Solutions
You may want to see also
Explore related products





![]()
Storage Guidelines: Proper storage of unused morphine to ensure safety and prevent diversion
Unused morphine presents a unique challenge in healthcare settings, balancing the need for accessibility with stringent safety and security measures. Proper storage is not just a regulatory requirement but a critical safeguard against diversion, misuse, and accidental exposure. Morphine’s potency and controlled substance status demand adherence to specific guidelines that go beyond standard medication storage protocols.
Steps for Secure Storage:
- Use Locked, Tamper-Evident Containers: Store unused morphine in a locked cabinet or safe accessible only to authorized personnel. Containers should be tamper-evident, with seals or locks that indicate unauthorized access.
- Maintain a Controlled Environment: Keep morphine at room temperature (59°F–86°F or 15°C–30°C) in its original packaging to protect it from light, moisture, and temperature extremes. Liquid morphine, such as oral solutions, should be stored upright to prevent leakage.
- Document Every Interaction: Implement a double-check system for accessing stored morphine. Log all withdrawals and returns, including date, time, dosage (e.g., 10 mg vials or 5 mg/mL solutions), and personnel involved. This creates an audit trail to detect discrepancies.
Cautions to Prevent Diversion:
Morphine’s high potential for abuse requires proactive measures to minimize diversion risks. Avoid storing large quantities; instead, maintain only the amount needed for immediate patient care. Regularly reconcile inventory against administration records, investigating any variances promptly. Educate staff on recognizing signs of diversion, such as frequent requests for morphine or discrepancies in waste documentation.
Practical Tips for Healthcare Settings:
In pediatric or geriatric units, where lower dosages (e.g., 0.1 mg/kg for children or 2.5 mg for elderly patients) are common, label storage areas clearly to prevent accidental administration of higher concentrations. Use color-coded containers or labels to distinguish morphine from other opioids. For home healthcare, advise caregivers to store morphine in a locked box out of reach of children and pets, disposing of unused medication through authorized take-back programs.
Proper storage of unused morphine is a multifaceted responsibility that protects patients, staff, and the public. By combining secure storage practices, vigilant documentation, and proactive diversion prevention, healthcare providers can ensure morphine remains a safe and effective tool for pain management while minimizing its risks.
Synthetic Plastic's Environmental Impact: Unraveling the Global Waste Crisis
You may want to see also
Explore related products






![]()
Witness Protocols: Requirement for a witness during the wasting process to ensure transparency
In healthcare settings, the wasting of unused morphine is a critical procedure governed by strict regulations to prevent diversion and ensure patient safety. One emerging best practice is the implementation of witness protocols, which mandate the presence of a second authorized individual during the wasting process. This requirement serves as a safeguard against errors, fraud, and misuse, fostering transparency and accountability in controlled substance management.
Consider the typical scenario: a nurse prepares to waste 5 mg of unused morphine from a 10 mg vial after administering the required dose to a patient. Without a witness, the process relies solely on the nurse’s documentation, leaving room for human error or intentional discrepancies. By requiring a witness—often another nurse or pharmacist—the act of wasting becomes a collaborative, verifiable event. The witness observes the measurement, confirms the amount being wasted, and co-signs the documentation, creating a dual-layered accountability system. This protocol is particularly crucial in high-risk environments like intensive care units or palliative care, where morphine usage is frequent and dosages are often titrated to patient needs.
Implementing witness protocols requires clear guidelines and training. For instance, the witness should be familiar with the proper wasting procedure, including the use of a controlled substance waste bin and the documentation of the exact volume wasted. In pediatric settings, where morphine dosages are weight-based (e.g., 0.05–0.2 mg/kg), precision is paramount, and a witness can help verify calculations and measurements. Hospitals may also adopt technological aids, such as video recording or digital verification systems, to supplement human observation, though these should not replace the real-time oversight of a trained professional.
Critics might argue that witness protocols add time and complexity to an already demanding workflow. However, the benefits outweigh the inconveniences. A study in a large urban hospital found that witness protocols reduced documentation errors by 40% and increased staff confidence in controlled substance handling. Moreover, the presence of a witness acts as a deterrent to potential misuse, aligning with DEA regulations and institutional compliance goals. For facilities adopting this practice, it is essential to integrate witness protocols into existing workflows, such as during shift changes or medication rounds, to minimize disruption.
In conclusion, witness protocols are not merely a regulatory checkbox but a cornerstone of ethical and safe morphine management. By requiring a second pair of eyes during the wasting process, healthcare institutions can uphold transparency, reduce risks, and maintain public trust. As the healthcare landscape evolves, such protocols will likely become standard practice, ensuring that every drop of unused morphine is accounted for—accurately, securely, and without exception.
Sustainable Living: Eliminating Waste from Living and Nonliving Sources
You may want to see also
Frequently asked questions
Yes, unused morphine must be wasted according to facility policies and regulatory guidelines, typically after administration is complete or if it exceeds the allowed time frame for use.
No, unused morphine cannot be saved for future use due to safety, regulatory, and infection control concerns. It must be properly discarded as waste.
The healthcare professional who draws up the morphine is typically responsible for ensuring it is properly wasted if unused, following the facility’s protocols and witnessing requirements.































