The glomerulus, a key component of the nephron in the kidney, plays a crucial role in the filtration of blood to remove waste products and excess fluids from the body. While the glomerulus primarily acts as a non-selective filter, allowing small molecules like water, ions, and waste products to pass through its porous structure, the process of waste removal is not entirely passive. Emerging research suggests that specific transport proteins may be involved in facilitating the movement of certain waste molecules across the glomerular barrier. These proteins could enhance the efficiency of waste removal, ensuring that harmful substances are effectively cleared from the bloodstream. Understanding the role of these transport proteins is essential for unraveling the intricate mechanisms of renal filtration and may provide insights into the development of targeted therapies for kidney diseases.
| Characteristics | Values |
|---|---|
| Use of Specific Transport Proteins | The glomerulus primarily relies on size and charge selectivity for waste removal, rather than specific transport proteins. |
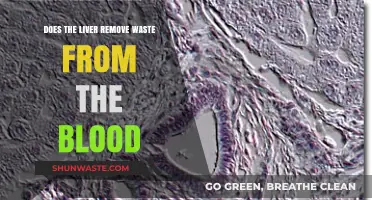
| Filtration Mechanism | Ultrafiltration occurs through the glomerular basement membrane and slit diaphragms of podocytes, which act as a size-selective barrier. |
| Size Selectivity | Molecules smaller than the cutoff size (approximately 70 kDa) are freely filtered, including waste products like urea, creatinine, and small ions. |
| Charge Selectivity | The glomerular barrier has a slight negative charge, which restricts the filtration of negatively charged molecules, though this is not a primary mechanism for waste removal. |
| Role of Transport Proteins | Specific transport proteins are not involved in the initial filtration process in the glomerulus. However, proximal tubule cells in the nephron use transport proteins (e.g., organic anion transporters, multidrug resistance proteins) to actively secrete waste products from the blood into the tubular lumen. |
| Waste Removal Efficiency | The glomerulus filters approximately 125 mL/min of plasma, effectively removing small waste molecules while retaining larger proteins and blood cells. |
| Regulation of Filtration | Filtration is regulated by glomerular hydrostatic pressure, capsular hydrostatic pressure, and glomerular oncotic pressure, not by transport proteins. |
| Comparison to Other Structures | Unlike the proximal tubule, which uses transport proteins for active secretion, the glomerulus is a passive filtration device. |
| Clinical Relevance | Dysfunction in glomerular filtration (e.g., due to damage to the basement membrane or podocytes) can lead to proteinuria or reduced waste clearance, but this is not related to transport proteins in the glomerulus itself. |
Explore related products






What You'll Learn
- Role of megalin and cubilin in proximal tubule endocytosis
- Function of organic anion transporters (OATs) in waste filtration
- Importance of sodium-glucose cotransporters (SGLTs) in glucose reabsorption
- Role of aquaporins in water movement across glomerular capillaries
- Contribution of multidrug resistance proteins (MRPs) in toxin secretion
![]()
Role of megalin and cubilin in proximal tubule endocytosis
The glomerulus, a key component of the kidney's filtration system, primarily acts as a sieve, allowing small molecules like waste products to pass into the tubules while retaining larger proteins and blood cells. However, the proximal tubule, the next segment in the nephron, plays a critical role in reclaiming essential molecules and further refining waste removal. Here, megalin and cubilin emerge as pivotal players in endocytosis, a process essential for the selective reabsorption and disposal of filtered substances.
Megalin, a large transmembrane receptor, acts as a molecular trap, binding to a diverse array of ligands, including proteins, hormones, and vitamins. Its broad specificity allows it to capture both essential molecules for reabsorption and waste products for elimination. Cubilin, another key player, functions as a co-receptor, enhancing megalin's ligand-binding capacity and facilitating the formation of endocytic vesicles. Together, they form a dynamic duo, ensuring that the proximal tubule efficiently processes the glomerular filtrate.
Consider the process as a highly organized recycling center. Megalin acts as the sorting conveyor belt, identifying and capturing items of interest, while cubilin assists in bundling these items for further processing. This coordinated effort is crucial for maintaining homeostasis, as it prevents the loss of valuable nutrients and ensures the removal of harmful waste products. For instance, megalin-mediated endocytosis is responsible for the reabsorption of up to 90% of filtered low-molecular-weight proteins, which are essential for bodily functions but would otherwise be lost in the urine.
Clinically, defects in megalin or cubilin function can lead to severe disorders, such as Lowe syndrome or Donnai-Barrow syndrome, characterized by impaired nutrient reabsorption and abnormal waste clearance. Understanding these proteins' roles provides insights into potential therapeutic targets for kidney diseases. For example, modulating megalin activity could offer a strategy to enhance the clearance of toxic proteins in conditions like multiple myeloma, where excessive light chains burden the kidneys.
In practical terms, researchers and clinicians can leverage knowledge of megalin and cubilin to develop diagnostic tools or therapies. For instance, measuring urinary levels of megalin-bound ligands could serve as a biomarker for proximal tubule dysfunction. Additionally, designing drugs that target these receptors could improve the treatment of kidney diseases by optimizing waste removal and nutrient retention. By focusing on these specific transport proteins, we unlock new avenues for addressing renal health challenges.
Exploring the Origins of Wasted on LoL: A Historical Journey
You may want to see also
Explore related products





![]()
Function of organic anion transporters (OATs) in waste filtration
Organic anion transporters (OATs) play a pivotal role in the kidney's waste filtration process, specifically within the proximal tubule, a critical site for reabsorption and secretion. These transporters are essential for eliminating a diverse array of organic anions, including toxins, drugs, and metabolic byproducts, from the bloodstream. Unlike the glomerulus, which primarily filters small molecules through size-based mechanisms, OATs provide a specialized pathway for larger, charged molecules that would otherwise evade filtration. This distinction highlights the kidney’s dual strategy: passive filtration in the glomerulus and active secretion in the proximal tubule, where OATs reside.
Consider the example of penicillin, a common antibiotic. When administered, penicillin is actively secreted into the proximal tubule lumen via OATs, ensuring its efficient removal from the body. This process is not passive; it requires energy and is highly selective, relying on OATs to recognize and transport specific substrates. Similarly, endogenous waste products like urate and cGMP are also cleared through these transporters, underscoring their role in maintaining metabolic homeostasis. Without functional OATs, such compounds could accumulate, leading to toxicity or metabolic disorders.
The clinical relevance of OATs cannot be overstated, particularly in pharmacology. Many drugs, including nonsteroidal anti-inflammatory drugs (NSAIDs) and antiviral agents, are substrates for OATs. For instance, the NSAID diclofenac relies on OATs for renal excretion. However, drug-drug interactions can inhibit OAT function, altering drug clearance and potentially leading to adverse effects. Patients with reduced OAT activity, whether due to genetic polymorphisms or disease, may require dosage adjustments to avoid toxicity. For example, a patient with chronic kidney disease might need a 25–50% reduction in diclofenac dosage to account for impaired OAT-mediated secretion.
To optimize waste filtration and drug safety, healthcare providers should consider OAT function when prescribing medications. Practical tips include avoiding co-administration of OAT inhibitors (e.g., probenecid) with OAT-dependent drugs, monitoring renal function in at-risk populations (e.g., the elderly or those with pre-existing kidney disease), and educating patients about the importance of adhering to prescribed dosages. Additionally, emerging research into OAT modulators offers potential for therapeutic interventions, such as enhancing the excretion of toxic compounds or improving drug efficacy.
In conclusion, OATs are indispensable for the kidney’s waste filtration system, bridging the gap left by the glomerulus’s size-based filtration. Their role in clearing organic anions, both endogenous and exogenous, is vital for health and drug management. Understanding OAT function allows for more precise clinical decision-making, ensuring safer and more effective treatment strategies. As research progresses, targeting OATs may unlock new avenues for managing renal disease and optimizing pharmacotherapy.
Waste King 8000 Power Cord Length: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Importance of sodium-glucose cotransporters (SGLTs) in glucose reabsorption
The glomerulus, a key player in kidney function, filters blood to remove waste while retaining essential nutrients like glucose. This process relies heavily on specific transport proteins, among which sodium-glucose cotransporters (SGLTs) are pivotal. SGLTs facilitate the reabsorption of glucose in the proximal tubule, ensuring that this vital energy source is not lost in urine. Without these transporters, glucose would be excreted, leading to energy depletion and potential metabolic disorders. Understanding SGLTs is crucial for appreciating the kidney's role in maintaining glucose homeostasis and for developing targeted therapies for conditions like diabetes.
SGLTs operate through a coupled transport mechanism, leveraging the sodium gradient across cell membranes. Specifically, SGLT2, located in the early proximal tubule, reabsorbs approximately 90% of filtered glucose, while SGLT1, found in the late proximal tubule and other tissues, handles the remaining 10%. This division of labor ensures efficient glucose recovery under normal conditions. For instance, in a healthy adult, the kidneys filter about 180 grams of glucose daily, nearly all of which is reabsorbed via SGLTs. This efficiency highlights their indispensable role in energy conservation and metabolic stability.
Clinically, SGLT inhibitors, such as empagliflozin and dapagliflozin, have emerged as transformative therapies for type 2 diabetes. By blocking SGLT2, these drugs promote glucose excretion, lowering blood sugar levels. A typical starting dose of empagliflozin is 10 mg daily, which can be increased to 25 mg for better glycemic control. However, their use requires caution in patients with impaired kidney function or dehydration risk, as they can exacerbate volume depletion. This dual role of SGLTs—both as essential physiological mediators and therapeutic targets—underscores their significance in glucose management.
Comparatively, SGLTs differ from other transport proteins in their specificity and energy efficiency. Unlike active transporters that rely on ATP, SGLTs harness the electrochemical sodium gradient, making them highly energy-efficient. This unique mechanism allows the kidneys to reabsorb glucose even under low-energy conditions, such as during fasting. In contrast, disorders like Fanconi syndrome, where generalized proximal tubule dysfunction occurs, highlight the consequences of impaired glucose reabsorption. Such conditions emphasize the critical role of SGLTs in preventing glycosuria and maintaining metabolic health.
In practical terms, monitoring SGLT function is essential for diagnosing and managing renal glucose handling disorders. For example, a random urine glucose test, combined with blood glucose levels, can identify glycosuria, a hallmark of SGLT dysfunction or inhibition. Patients on SGLT2 inhibitors should monitor for symptoms of dehydration and ketoacidosis, particularly in older adults or those with comorbidities. Additionally, dietary considerations, such as maintaining adequate fluid intake and avoiding excessive sugar consumption, can support optimal SGLT function. By recognizing the importance of SGLTs, healthcare providers can better address glucose-related disorders and optimize patient outcomes.
Porifera's Metabolic Waste Excretion: A Unique Cellular Process Explained
You may want to see also
Explore related products






![]()
Role of aquaporins in water movement across glomerular capillaries
Aquaporins, a family of transmembrane proteins, play a pivotal role in facilitating water movement across biological membranes, including those of glomerular capillaries. These proteins form channels that allow water to pass through cell membranes at a rate far exceeding simple diffusion, a process critical for maintaining fluid balance in the body. In the context of the glomerulus, aquaporins are specifically expressed in the endothelial cells lining the capillaries, where they enable rapid water movement from the blood into the Bowman's capsule, a key step in urine formation. This process is essential for efficient waste removal, as it ensures that water follows solutes filtered out of the blood, preventing osmotic imbalances.
The primary aquaporin involved in glomerular filtration is AQP1, which is highly expressed in the endothelial cells of the glomerular capillaries. Studies have shown that AQP1 knockout mice exhibit reduced glomerular filtration rates, highlighting its importance in maintaining proper kidney function. The protein’s presence ensures that water movement is not a limiting factor in filtration, allowing the glomerulus to handle the large volumes of fluid processed daily. For instance, in humans, the kidneys filter approximately 180 liters of water per day, a task that would be impossible without the efficient water transport facilitated by aquaporins.
From a practical standpoint, understanding the role of aquaporins in glomerular filtration has implications for diagnosing and treating kidney disorders. Conditions such as nephrogenic diabetes insipidus, where mutations in aquaporin genes impair water reabsorption, underscore the protein’s clinical significance. Additionally, pharmacological agents targeting aquaporins are being explored as potential therapies for conditions like hypertension and edema, where regulating water balance is critical. For example, AQP1 inhibitors are being investigated for their ability to reduce excessive fluid filtration in certain disease states.
Comparatively, while other transport proteins in the glomerulus, such as those involved in solute reabsorption, are equally important, aquaporins stand out due to their specificity for water. Unlike solute transporters, which are selective for specific molecules like glucose or ions, aquaporins exclusively facilitate water movement, making them uniquely suited to their role. This specificity ensures that water follows the osmotic gradients established by solute filtration, a process vital for maintaining the concentration gradient necessary for waste removal.
In conclusion, aquaporins, particularly AQP1, are indispensable for efficient water movement across glomerular capillaries, a process central to kidney function and waste removal. Their role in facilitating rapid water transport ensures that the glomerulus can effectively filter blood while maintaining fluid balance. Clinically, understanding aquaporins opens avenues for targeted therapies and highlights their importance in both health and disease. By focusing on these proteins, researchers and clinicians can develop more precise interventions to address disorders of water balance and kidney function.
Internal Combustion Engines: Uncovering the Environmental Impact of Their Waste
You may want to see also
Explore related products






![]()
Contribution of multidrug resistance proteins (MRPs) in toxin secretion
Multidrug resistance proteins (MRPs), primarily known for their role in drug efflux, are increasingly recognized as key players in toxin secretion within the glomerulus. These ATP-binding cassette (ABC) transporters, particularly MRP2 and MRP4, are expressed in the apical membrane of proximal tubule cells, facilitating the removal of endogenous and exogenous toxins from the bloodstream. For instance, MRP2 is crucial for the elimination of bilirubin glucuronides, while MRP4 handles organic anions like cyclic nucleotides. This specificity underscores their importance in renal waste management, acting as a protective barrier against systemic toxicity.
To understand their contribution, consider the process of toxin secretion as a multi-step filtration system. First, toxins are filtered through the glomerulus into the tubule lumen. Next, MRPs in the proximal tubule cells actively transport these toxins from the cytoplasm into the urine, preventing their reabsorption. This mechanism is particularly vital for lipophilic toxins, which would otherwise accumulate in tissues. For example, in cases of drug-induced nephrotoxicity, MRPs can mitigate damage by expelling harmful compounds like cisplatin metabolites. However, their activity is dose-dependent; excessive toxin exposure may overwhelm MRP capacity, highlighting the need for balanced renal function.
Clinically, the role of MRPs in toxin secretion has implications for drug dosing and patient management. In pediatric populations, where renal function is still maturing, MRP activity may be suboptimal, necessitating lower drug dosages to avoid toxicity. Conversely, in elderly patients, age-related decline in MRP expression can impair toxin clearance, requiring careful monitoring. Practical tips include assessing renal function before prescribing MRP substrates and considering alternative therapies in patients with compromised MRP activity. For instance, in cases of Gilbert’s syndrome, where MRP2 function is impaired, bilirubin levels must be closely monitored to prevent complications.
Comparatively, MRPs differ from other renal transporters like P-glycoprotein (P-gp) in their substrate specificity and localization. While P-gp primarily handles cationic drugs, MRPs focus on anionic and organic toxins. This distinction makes MRPs indispensable for clearing a unique subset of waste products. However, their overlap with other transporters in certain substrates, such as prostaglandins, highlights the complexity of renal toxin handling. Understanding these interactions is crucial for developing targeted therapies that enhance MRP activity without disrupting other transport pathways.
In conclusion, MRPs are not merely drug resistance proteins but essential contributors to renal toxin secretion. Their role in protecting the body from harmful substances is both specific and critical, particularly in vulnerable populations. By optimizing their function through tailored drug regimens and monitoring, healthcare providers can enhance renal waste management and reduce toxicity risks. This knowledge bridges the gap between basic science and clinical practice, offering actionable insights for improved patient outcomes.
Transforming Waste into Power: Sustainable Energy Solutions for a Greener Future
You may want to see also
Frequently asked questions
No, the glomerulus primarily relies on passive filtration driven by hydrostatic pressure to remove waste products from the blood. Specific transport proteins are not involved in this process.
The glomerulus uses a size- and charge-selective barrier, composed of the glomerular basement membrane, podocytes, and endothelial cells, to filter waste based on molecular size and charge, rather than specific transport proteins.
Yes, transport proteins are involved in the reabsorption and secretion processes in the renal tubules, not the glomerulus. These proteins help regulate the final composition of urine after filtration.