The kidneys play a crucial role in maintaining homeostasis by filtering blood, removing waste products, and regulating fluid and electrolyte balance. During the filtration process, blood passes through the glomeruli, where small molecules like water, electrolytes, and waste products are filtered into the nephron tubules. However, not all filtered substances are destined for excretion; the kidneys selectively reabsorb essential molecules such as glucose, amino acids, and certain electrolytes back into the bloodstream. The question of whether the kidneys reabsorb filtered waste products is particularly intriguing, as it challenges the conventional understanding of renal function. While the primary purpose of the kidneys is to eliminate waste, recent studies suggest that certain waste products, under specific physiological conditions, may undergo limited reabsorption, raising questions about the mechanisms and implications of this process. Understanding this phenomenon is essential for comprehending renal physiology and its potential impact on health and disease.
| Characteristics | Values |
|---|---|
| Reabsorption of Filtered Waste Products | The kidneys do not typically reabsorb filtered waste products. Instead, they selectively reabsorb essential substances like glucose, amino acids, and water, while allowing waste products (e.g., urea, creatinine) to remain in the filtrate for excretion. |
| Selective Reabsorption | Occurs primarily in the proximal tubule, loop of Henle, and distal tubule, where specific transporters and channels facilitate the reabsorption of useful substances. |
| Waste Excretion | Waste products are excreted in the urine after passing through the nephron and collecting duct, ensuring they are removed from the body. |
| Role of Active Transport | Essential substances are reabsorbed via active transport mechanisms, while waste products are passively filtered and not actively reabsorbed. |
| Regulation by Hormones | Hormones like antidiuretic hormone (ADH) and aldosterone regulate water and electrolyte reabsorption but do not affect waste product reabsorption. |
| Clinical Relevance | Impaired reabsorption of essential substances can lead to conditions like diabetes insipidus, while failure to excrete waste products results in conditions like uremia. |
Explore related products





What You'll Learn
- Proximal Tubule Reabsorption: Reabsorbs majority of filtered nutrients, water, and solutes, including glucose and amino acids
- Loop of Henle Function: Regulates water and ion balance, reabsorbing sodium and chloride passively
- Distal Tubule Role: Fine-tunes electrolyte balance, reabsorbing sodium and secreting potassium and hydrogen ions
- Collecting Duct Action: Adjusts water reabsorption based on antidiuretic hormone (ADH) levels
- Selective Reabsorption: Ensures essential substances return to blood while waste remains in urine
![]()
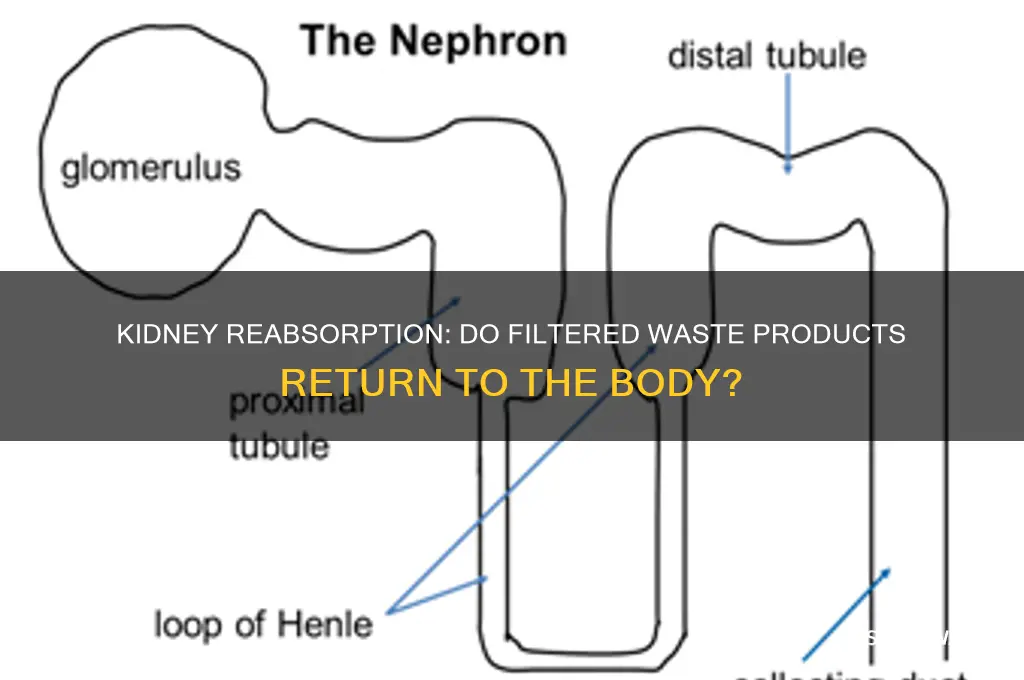
Proximal Tubule Reabsorption: Reabsorbs majority of filtered nutrients, water, and solutes, including glucose and amino acids
The proximal tubule, often referred to as the workhorse of the nephron, plays a pivotal role in renal physiology by reabsorbing approximately 65-70% of filtered water, sodium, and chloride, along with nearly 100% of filtered glucose, amino acids, and other essential solutes. This process is not passive but actively regulated, primarily driven by sodium-glucose cotransporters (SGLT) and sodium-amino acid cotransporters. For instance, SGLT2 in the early proximal tubule reabsorbs the majority of glucose, ensuring that less than 0.1% of filtered glucose appears in the urine under normal conditions. This mechanism is so efficient that it serves as a diagnostic marker: glycosuria (glucose in urine) often indicates diabetes mellitus or SGLT2 dysfunction.
Consider the practical implications of this reabsorption process. In patients with diabetes, hyperglycemia exceeds the reabsorptive capacity of the proximal tubule, leading to glycosuria. Clinicians use this phenomenon to monitor glycemic control, with a urine glucose threshold of ≥180 mg/dL typically indicating renal threshold exceedance. Similarly, amino acid reabsorption is critical for maintaining protein homeostasis. Conditions like Fanconi syndrome, where proximal tubule dysfunction impairs reabsorption, result in aminoaciduria, glycosuria, and phosphate wasting. Early detection and management of such disorders rely on understanding the proximal tubule’s role, emphasizing its clinical significance.
From a comparative perspective, the proximal tubule’s reabsorption efficiency contrasts sharply with other nephron segments. While the loop of Henle and distal tubule fine-tune water and electrolyte balance, the proximal tubule handles the bulk of reabsorption, acting as the kidney’s primary filter for essential nutrients. This division of labor ensures that the body retains vital substances while allowing waste products to be excreted. For example, the proximal tubule reabsorbs bicarbonate ions, a process critical for acid-base balance, while the distal tubule secretes hydrogen ions to regulate pH. This interplay highlights the proximal tubule’s central role in both nutrient conservation and systemic homeostasis.
To optimize kidney health, individuals should be mindful of factors that impair proximal tubule function. Chronic conditions like hypertension and diabetes, as well as acute insults from nephrotoxic drugs (e.g., NSAIDs), can disrupt reabsorption mechanisms. Practical tips include maintaining euglycemia in diabetes, staying hydrated to support renal blood flow, and avoiding excessive use of over-the-counter medications that strain the kidneys. For older adults (≥65 years), regular monitoring of renal function (e.g., serum creatinine, eGFR) is essential, as age-related declines in proximal tubule efficiency increase susceptibility to electrolyte imbalances and drug toxicity. By safeguarding proximal tubule function, individuals can preserve renal health and overall well-being.
E-Waste Crisis: How Discarded Electronics Impact Human Health and Environment
You may want to see also
Explore related products






![]()
Loop of Henle Function: Regulates water and ion balance, reabsorbing sodium and chloride passively
The Loop of Henle, a critical component of the nephron in the kidney, is a marvel of biological engineering designed to regulate water and ion balance with precision. Unlike active transport mechanisms that require energy, the Loop of Henle primarily reabsorbs sodium and chloride passively, relying on concentration gradients established by surrounding structures. This process is fundamental to maintaining osmotic balance and ensuring proper hydration levels in the body. For instance, in the thick ascending limb of the Loop of Henle, sodium, potassium, and chloride are reabsorbed via a secondary active transport system, but the initial driving force remains passive, showcasing the kidney’s efficiency in conserving energy while performing vital functions.
To understand the Loop of Henle’s role in water and ion regulation, consider its unique structure: a hairpin-shaped tube divided into descending and ascending limbs. The descending limb is permeable to water but not ions, allowing water to move out of the filtrate into the surrounding interstitium, concentrating the urine. Conversely, the thick ascending limb is impermeable to water but actively reabsorbs sodium and chloride, diluting the interstitium. This countercurrent mechanism ensures that the medulla of the kidney remains hypertonic, a critical condition for water reabsorption in the collecting ducts later in the process. This system is particularly vital in environments where water conservation is essential, such as in desert-dwelling organisms.
From a practical standpoint, understanding the Loop of Henle’s function is crucial for managing conditions like hyponatremia or hypernatremia, where sodium and water balance are disrupted. For example, in patients with syndrome of inappropriate antidiuretic hormone (SIADH), excessive water reabsorption dilutes sodium levels in the blood. Clinicians often prescribe fluid restriction and, in severe cases, hypertonic saline (3% NaCl) at a rate of 1–2 mL/kg/hr to correct sodium levels gradually, avoiding rapid shifts that could harm the brain. Conversely, in hypernatremia, free water replacement is administered orally or intravenously, with dosages tailored to age and severity—typically 50–100 mL/kg/day for children and adjusted downward for adults.
Comparatively, the Loop of Henle’s passive reabsorption of ions contrasts with the proximal tubule’s active reabsorption processes, highlighting the kidney’s layered approach to filtration and reabsorption. While the proximal tubule reabsorbs approximately 65% of filtered sodium and water, the Loop of Henle fine-tunes this balance, ensuring that the body retains only what is necessary. This division of labor underscores the kidney’s ability to adapt to varying physiological demands, such as during dehydration or excessive fluid intake. For instance, in dehydration, antidiuretic hormone (ADH) enhances water reabsorption in the collecting ducts, but the Loop of Henle’s passive mechanisms remain active, maintaining ion balance without additional energy expenditure.
In conclusion, the Loop of Henle’s function in passively reabsorbing sodium and chloride is a cornerstone of renal physiology, enabling precise regulation of water and ion balance. Its unique structure and countercurrent mechanism exemplify nature’s ingenuity in solving complex biological challenges. For healthcare professionals and students alike, appreciating this process not only deepens understanding of kidney function but also informs practical interventions for electrolyte and fluid imbalances. Whether managing a patient with SIADH or teaching the principles of renal physiology, the Loop of Henle serves as a testament to the elegance and efficiency of the human body’s regulatory systems.
Does Exiting FIFA Matches Impact Your Coin Boost? Find Out
You may want to see also
Explore related products






![]()
Distal Tubule Role: Fine-tunes electrolyte balance, reabsorbing sodium and secreting potassium and hydrogen ions
The distal tubule, a seemingly modest segment of the nephron, plays a pivotal role in maintaining the body's delicate electrolyte equilibrium. Here, a sophisticated exchange process occurs, ensuring the precise regulation of sodium, potassium, and hydrogen ions. This fine-tuning is essential, as even slight deviations in electrolyte levels can have significant physiological consequences.
A Delicate Dance of Ions: Imagine a meticulous choreographer directing a complex dance, where each movement is critical to the overall performance. Similarly, the distal tubule orchestrates the reabsorption of sodium and the secretion of potassium and hydrogen ions. This process is not merely a passive filtration but an active, energy-dependent mechanism. The tubule cells utilize specific transporters and channels to facilitate this exchange, ensuring that the body's electrolyte composition remains within a narrow, healthy range. For instance, the sodium-chloride cotransporter (NCC) is a key player in sodium reabsorption, while the renal outer medullary potassium channel (ROMK) is crucial for potassium secretion.
Clinical Implications and Precision: Understanding this process is not just an academic exercise; it has direct clinical relevance. In certain medical conditions, such as hypertension or kidney disease, the distal tubule's function can be impaired. For example, in some forms of hypertension, the excessive reabsorption of sodium in the distal tubule contributes to elevated blood pressure. Here, medical interventions often target this specific mechanism. Diuretics, a class of drugs commonly used to treat hypertension, act by inhibiting sodium reabsorption in the distal tubule, thereby promoting sodium excretion and reducing blood volume. This highlights the importance of the distal tubule in maintaining not just electrolyte balance but also overall cardiovascular health.
A Comparative Perspective: To appreciate the distal tubule's role, consider the contrast with other nephron segments. While the proximal tubule is responsible for the bulk reabsorption of filtered substances, the distal tubule's function is more specialized and fine-tuned. It acts as a final regulator, making subtle adjustments to ensure the body's internal environment remains stable. This is particularly crucial in situations where dietary intake or physiological demands fluctuate. For instance, after a high-sodium meal, the distal tubule increases sodium excretion to prevent excessive retention, demonstrating its adaptive capabilities.
Practical Insights and Takeaways: For individuals, especially those with kidney health concerns, understanding this process can empower better dietary and lifestyle choices. Maintaining a balanced diet with adequate potassium-rich foods (e.g., bananas, spinach) and moderating sodium intake can support the distal tubule's function. Additionally, staying hydrated is essential, as it ensures optimal kidney function and facilitates the efficient removal of waste products. For patients with kidney disorders, regular monitoring of electrolyte levels and adherence to prescribed medications are vital to prevent complications. In summary, the distal tubule's role in fine-tuning electrolyte balance is a critical aspect of kidney function, with implications for overall health and disease management.
Vermont's 1990 Wastewater Regulations: Did Permits Become Mandatory?
You may want to see also
Explore related products






![]()
Collecting Duct Action: Adjusts water reabsorption based on antidiuretic hormone (ADH) levels
The collecting duct, a tiny yet pivotal player in kidney function, acts as a gatekeeper for water reabsorption, fine-tuning fluid balance in response to the body's needs. This process is orchestrated by antidiuretic hormone (ADH), also known as vasopressin, which is secreted by the hypothalamus and released by the posterior pituitary gland. When ADH levels are high, the collecting duct becomes more permeable to water, allowing for increased reabsorption and the production of concentrated urine. Conversely, low ADH levels result in reduced water reabsorption, leading to dilute urine and increased fluid excretion.
Consider a scenario where an individual is dehydrated, such as after intense exercise or during illness. In response, the body releases higher levels of ADH, typically ranging from 1 to 5 pg/mL in a dehydrated state compared to 0.5 to 2 pg/mL in a well-hydrated state. This surge in ADH binds to V2 receptors on the basolateral membrane of collecting duct cells, activating a signaling cascade that inserts aquaporin-2 (AQP2) water channels into the apical membrane. These channels facilitate the rapid movement of water from the lumen of the collecting duct back into the bloodstream, conserving fluid and maintaining homeostasis.
To optimize kidney function and support this mechanism, practical steps can be taken. For instance, staying adequately hydrated by consuming 8–10 cups of water daily helps maintain baseline ADH levels. However, in cases of severe dehydration, medical intervention may be necessary, such as the administration of synthetic ADH analogs like desmopressin (DDAVP), typically prescribed at doses of 0.1 to 0.2 mg for adults. It’s crucial to monitor sodium levels during such treatments, as excessive water reabsorption can lead to hyponatremia, a dangerous condition characterized by low blood sodium levels.
Comparatively, conditions like diabetes insipidus highlight the critical role of ADH in collecting duct function. In this disorder, either insufficient ADH production (central diabetes insipidus) or kidney resistance to ADH (nephrogenic diabetes insipidus) results in the inability to concentrate urine, leading to excessive urination and thirst. Treatment strategies differ: central diabetes insipidus often requires desmopressin therapy, while nephrogenic diabetes insipidus may involve medications like thiazide diuretics or nonsteroidal anti-inflammatory drugs to enhance ADH responsiveness.
In essence, the collecting duct’s response to ADH is a dynamic, finely tuned process that ensures fluid balance under varying physiological conditions. Understanding this mechanism not only sheds light on normal kidney function but also provides insights into managing disorders related to water reabsorption. By recognizing the interplay between ADH levels and collecting duct action, individuals and healthcare providers can take targeted steps to support kidney health and overall well-being.
Does Oven Decarboxylation Waste Bud? Facts and Best Practices
You may want to see also
Explore related products





![]()
Selective Reabsorption: Ensures essential substances return to blood while waste remains in urine
The kidneys are master chemists, meticulously regulating the body's internal environment. One of their most crucial functions is selective reabsorption, a process akin to a bouncer at an exclusive club, allowing only essential substances back into the bloodstream while keeping waste products out. This intricate mechanism ensures that vital nutrients, electrolytes, and water are retained, while toxins and excess substances are eliminated in urine.
Understanding the Mechanism
Imagine a highly efficient filtration system. Blood enters the kidney's nephrons, where it's filtered under pressure, separating smaller molecules like glucose, amino acids, and electrolytes from larger proteins and blood cells. This filtrate then passes through a series of specialized tubules. Here, the magic of selective reabsorption occurs. Specific transport proteins embedded in the tubule walls act as gatekeepers, recognizing and actively transporting essential substances back into the bloodstream. This process is tightly regulated by hormones like antidiuretic hormone (ADH) and aldosterone, which fine-tune the reabsorption of water and electrolytes based on the body's needs.
Consequences of Dysfunction
When selective reabsorption falters, the consequences can be severe. Diabetes insipidus, for example, arises from a deficiency in ADH, leading to excessive urination and dehydration as water is not adequately reabsorbed. Conversely, conditions like hyperkalemia (high potassium levels) can occur if potassium reabsorption is impaired, potentially causing cardiac arrhythmias. Understanding these mechanisms highlights the delicate balance maintained by the kidneys and the importance of proper kidney function for overall health.
Practical Implications
For individuals with kidney disease or those at risk, monitoring electrolyte levels and fluid balance becomes crucial. Dietary modifications, such as reducing sodium intake to manage blood pressure or limiting potassium-rich foods in cases of impaired potassium excretion, can support kidney function. Additionally, medications like diuretics, which alter water and electrolyte reabsorption, must be used judiciously, considering their impact on this delicate process. Regular check-ups and blood tests can help detect early signs of dysfunction, allowing for timely intervention.
The Future of Kidney Health
Advances in medical research are shedding light on the intricate molecular mechanisms of selective reabsorption, paving the way for targeted therapies. For instance, developing drugs that modulate specific transport proteins could offer more precise treatments for conditions like chronic kidney disease. Furthermore, regenerative medicine approaches, such as growing functional kidney tissue in the lab, hold promise for restoring selective reabsorption capabilities in damaged kidneys. As our understanding deepens, we move closer to a future where kidney health is not just maintained but optimized.
Reducing Food Waste: Understanding Grain Product Loss and Solutions
You may want to see also
Frequently asked questions
No, the kidneys do not reabsorb filtered waste products. Instead, they selectively reabsorb essential substances like water, glucose, and electrolytes while allowing waste products to remain in the filtrate for eventual excretion in urine.
During kidney filtration, waste products such as urea, creatinine, and excess ions are filtered out of the blood into the nephron. These waste products are not reabsorbed and are excreted in urine.
The kidneys do not reabsorb filtered waste products because their primary function is to eliminate these substances from the body. Reabsorbing waste would defeat the purpose of filtration and detoxification.
The kidneys reabsorb essential substances like water, glucose, amino acids, and electrolytes (e.g., sodium, potassium) that the body needs to maintain homeostasis, rather than waste products.
The kidneys ensure waste products are not reabsorbed through selective permeability in the proximal tubule and other nephron segments. Waste products are actively secreted or passively retained in the filtrate for excretion.