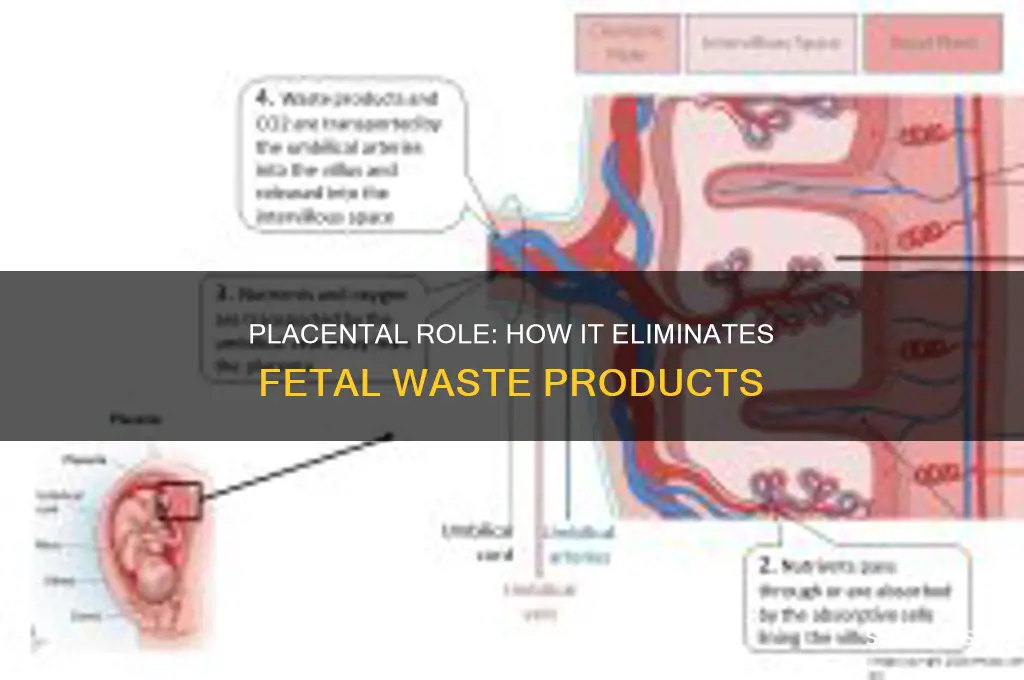
The placenta is a vital organ that plays a crucial role in fetal development, acting as the primary interface between the mother and the fetus. One of its key functions is to facilitate the exchange of nutrients, oxygen, and waste products, ensuring the fetus receives essential resources while eliminating harmful byproducts. Among its many responsibilities, the placenta is indeed responsible for removing waste products from the fetus, such as carbon dioxide and urea, which are generated as a result of fetal metabolism. These waste products are transferred from the fetal bloodstream to the maternal bloodstream through the placenta, where they can be safely eliminated by the mother's body, thereby maintaining a healthy and stable environment for the developing fetus.
| Characteristics | Values |
|---|---|
| Primary Function | Facilitates exchange of nutrients, oxygen, and waste products between maternal and fetal blood. |
| Waste Removal Mechanism | Yes, the placenta removes fetal waste products such as carbon dioxide, urea, and other metabolic byproducts. |
| Process of Waste Exchange | Waste products diffuse from fetal blood into maternal blood through the placental barrier. |
| Maternal Blood Role | Transports fetal waste products to the mother's kidneys and lungs for elimination. |
| Key Waste Products Removed | Carbon dioxide (CO₂), urea, and other nitrogenous wastes. |
| Placental Barrier | Prevents direct mixing of maternal and fetal blood while allowing exchange of gases and waste. |
| Importance of Waste Removal | Essential for maintaining fetal homeostasis and preventing toxicity from waste accumulation. |
| Related Maternal Organs | Mother's kidneys (for urea excretion) and lungs (for CO₂ excretion). |
| Developmental Stage | Placenta begins waste removal function early in pregnancy and continues until birth. |
| Clinical Significance | Placental dysfunction can lead to fetal waste accumulation, causing conditions like fetal acidosis. |
Explore related products



$46.69 $57.99


![Hair loss Placenta Placo for hair intensive treatment [12 vials 0,35 oz]](https://m.media-amazon.com/images/I/61IfSge-WcL._AC_UL320_.jpg)
What You'll Learn
![]()
Placental barrier function and waste filtration
The placenta, a temporary organ connecting the fetus to the mother, is a marvel of biological engineering. One of its critical functions is acting as a selective barrier, regulating the exchange of substances between maternal and fetal blood. This barrier is not just a passive filter but an active interface that ensures the fetus receives essential nutrients and oxygen while preventing harmful substances from crossing over. Waste filtration is a key aspect of this process, as the placenta must efficiently remove metabolic byproducts generated by the fetus to maintain a healthy intrauterine environment.
Consider the fetus’s primary waste products: carbon dioxide, urea, and creatinine. These are produced as a result of fetal metabolism and must be eliminated to prevent toxicity. The placental barrier facilitates this removal through a combination of diffusion and active transport mechanisms. Carbon dioxide, for instance, diffuses from fetal blood, which has a higher concentration, to maternal blood, where it is then exhaled by the mother. Urea and creatinine, on the other hand, are actively transported across the placental membrane into the maternal circulation, where they are filtered by the mother’s kidneys and excreted in urine. This dual system ensures that waste does not accumulate in the fetal compartment.
However, the placental barrier is not infallible. Its efficiency can be compromised by factors such as maternal health conditions (e.g., diabetes, hypertension), substance use (e.g., smoking, alcohol), or placental insufficiency. For example, in cases of maternal diabetes, elevated glucose levels can lead to increased fetal insulin production, resulting in larger fetal size and higher metabolic waste generation. If the placenta cannot keep up with the increased waste load, it may lead to fetal distress or complications like macrosomia. Similarly, toxins like nicotine or alcohol can cross the placenta, overwhelming its filtration capacity and exposing the fetus to harm.
To optimize placental waste filtration, expectant mothers should prioritize a healthy lifestyle. Maintaining stable blood sugar levels through balanced nutrition and regular monitoring is crucial for diabetic mothers. Avoiding smoking, alcohol, and illicit drugs is non-negotiable, as these substances not only cross the placenta but also impair its function. Regular prenatal check-ups are essential to monitor placental health and address any issues early. For instance, Doppler ultrasound can assess placental blood flow, providing insights into its efficiency in waste removal.
In summary, the placental barrier’s role in waste filtration is a delicate yet vital process that sustains fetal well-being. While it is highly efficient under normal conditions, external factors can compromise its function, underscoring the importance of maternal health and lifestyle choices. By understanding this mechanism, healthcare providers and expectant parents can take proactive steps to ensure the placenta performs its role optimally, safeguarding the developing fetus from metabolic waste accumulation and its associated risks.
Is the Department of Transportation Mismanaging Taxpayer Funds?
You may want to see also
Explore related products






![]()
Transfer of fetal metabolic waste to maternal blood
The placenta, a temporary organ connecting the fetus to the maternal uterus, plays a critical role in waste removal. Fetal metabolic waste, primarily carbon dioxide, urea, and creatinine, must be efficiently transferred to the maternal bloodstream for elimination. This process is essential because the fetal lungs are non-functional for gas exchange, and the developing kidneys have limited capacity for waste filtration. The placenta acts as a selective barrier, allowing waste products to diffuse from fetal to maternal blood while preventing the passage of harmful substances.
Mechanisms of Waste Transfer
Passive diffusion drives the movement of carbon dioxide and oxygen across the placental membrane, facilitated by the concentration gradient between fetal and maternal blood. Urea and creatinine, end products of protein metabolism, also diffuse into the maternal circulation due to their small molecular size. This diffusion is highly efficient, ensuring that fetal waste levels remain within safe physiological ranges. For instance, fetal blood urea nitrogen (BUN) levels are maintained at approximately 5-10 mg/dL, mirroring maternal levels, thanks to this continuous exchange.
Clinical Implications and Monitoring
In cases of placental insufficiency or maternal kidney dysfunction, fetal waste clearance can be compromised. Elevated fetal BUN or creatinine levels may indicate reduced placental function or maternal renal impairment. Clinicians monitor these parameters through amniocentesis or ultrasound assessments, particularly in high-risk pregnancies. For example, a BUN level exceeding 20 mg/dL in the fetus may warrant further investigation into placental or maternal health.
Practical Tips for Optimal Waste Clearance
Maternal hydration is crucial for maintaining adequate blood flow to the placenta, ensuring efficient waste removal. Pregnant individuals should aim for 2.3 to 3 liters of water daily, adjusting for activity level and climate. Avoiding substances that impair kidney function, such as excessive protein intake or nephrotoxic medications, is equally important. Regular prenatal check-ups, including urine analysis and blood tests, help identify potential issues early, allowing for timely intervention to support both maternal and fetal health.
Comparative Perspective
Unlike the adult kidney, which actively filters waste, the placenta relies on passive mechanisms for waste transfer. This distinction highlights the placenta’s unique role as a temporary waste management system. While the fetal kidneys contribute minimally to waste excretion, they gradually mature in preparation for postnatal function. Understanding this interplay between placental and fetal systems underscores the importance of maternal health in ensuring optimal waste clearance during pregnancy.
Worn Rotors and Fuel Efficiency: Are You Wasting Gas?
You may want to see also
Explore related products






![]()
Role of placental transporters in waste removal
The placenta, a temporary organ connecting the fetus to the maternal uterus, is a marvel of biological engineering. Among its many functions, waste removal is critical for fetal health. Placental transporters, specialized proteins embedded in its membranes, facilitate the movement of waste products from the fetal bloodstream to the maternal circulation. These transporters are not passive channels but active systems, selectively filtering out metabolic byproducts like urea, carbon dioxide, and lactic acid. Without this efficient waste disposal, toxic accumulation could impair fetal development, underscoring the placenta’s role as both a lifeline and a detoxifier.
Consider the transporter systems as gatekeepers, each with a specific function. Organic anion transporters (OATs) and multidrug resistance-associated proteins (MRPs) are key players in removing water-soluble waste products, such as urea and bilirubin. Meanwhile, carbonic anhydrases accelerate the conversion of carbon dioxide into bicarbonate, which diffuses into maternal blood. These processes are finely tuned to the fetal metabolic rate, increasing in efficiency as the fetus grows. For instance, by the third trimester, placental waste removal capacity peaks to handle the fetus’s heightened metabolic demands, ensuring a clean internal environment for growth.
Clinicians and researchers often draw parallels between placental transporters and renal systems, given their shared role in waste management. However, the placenta operates under unique constraints. Unlike kidneys, it must balance waste removal with nutrient delivery, all while preventing the transfer of harmful maternal substances. This dual responsibility highlights the sophistication of placental transporters, which must be both permeable and protective. Disruptions in these systems, often seen in conditions like preeclampsia or fetal growth restriction, can lead to waste accumulation, emphasizing their critical role in pregnancy outcomes.
Practical implications of understanding placental transporters extend to clinical care. For example, monitoring maternal urine output and fetal amniotic fluid levels can indirectly assess placental waste removal efficiency. Pregnant individuals with conditions like diabetes or hypertension may require closer surveillance, as these disorders can impair transporter function. Additionally, emerging research suggests that certain dietary interventions, such as adequate hydration and balanced protein intake, may support optimal transporter activity. While not a substitute for medical advice, these insights empower individuals to take proactive steps in promoting placental health.
In conclusion, placental transporters are unsung heroes in fetal waste removal, operating with precision and adaptability. Their role goes beyond mere filtration, embodying a delicate balance between protection and provision. By studying these mechanisms, we not only deepen our understanding of fetal physiology but also pave the way for targeted interventions to improve pregnancy outcomes. Whether in research or clinical practice, recognizing the importance of these transporters is essential for safeguarding fetal well-being.
Inside Waste Processing Plants: Transforming Trash into Resources Step-by-Step
You may want to see also
Explore related products






![]()
Urea and carbon dioxide elimination via placenta
The placenta, a temporary organ connecting the fetus to the mother, plays a critical role in waste elimination. Among the waste products it handles, urea and carbon dioxide are particularly significant. These metabolic byproducts, if allowed to accumulate, could pose serious risks to fetal development. Understanding how the placenta efficiently removes these substances is essential for appreciating its function in maintaining a healthy intrauterine environment.
Urea, a byproduct of protein metabolism, is produced by the fetus as it breaks down amino acids for growth and energy. Unlike the adult kidney, the fetal kidney is not fully equipped to excrete urea effectively. Instead, the placenta takes on this responsibility, acting as a filtration system. Urea diffuses from the fetal bloodstream into the maternal bloodstream through the placental barrier, a process driven by concentration gradients. Once in the maternal circulation, the mother’s kidneys filter and excrete the urea via urine. This mechanism ensures that fetal urea levels remain within safe limits, preventing toxicity that could impair fetal organ function.
Carbon dioxide (CO₂), a waste product of cellular respiration, is another critical substance the placenta helps eliminate. Fetal tissues produce CO₂ continuously, which dissolves into the fetal blood and is transported to the placenta. Here, CO₂ diffuses across the placental membrane into the maternal blood, where it binds to hemoglobin or is converted to bicarbonate. The mother’s respiratory system then expels the CO₂ with each exhale. This efficient exchange is vital, as elevated CO₂ levels in the fetus could lead to acidosis, a condition that disrupts fetal pH balance and potentially affects neurological development.
Comparing the elimination of urea and CO₂ highlights the placenta’s dual role as both a filter and an exchange interface. While urea removal relies on passive diffusion and maternal renal function, CO₂ elimination involves gas exchange mechanisms similar to those in the lungs. This duality underscores the placenta’s adaptability in managing diverse waste products. For instance, in cases of maternal kidney dysfunction, urea may accumulate in both mother and fetus, necessitating medical intervention such as dialysis. Similarly, maternal respiratory conditions like asthma can impair CO₂ elimination, emphasizing the interdependence of maternal and fetal health.
Practically, monitoring placental function is crucial for ensuring effective waste removal. Routine prenatal tests, such as ultrasound assessments of blood flow and fetal biophysical profiles, can detect abnormalities in placental efficiency. Pregnant individuals should maintain optimal hydration and kidney health to support urea excretion, while avoiding smoking or pollutants that could compromise respiratory CO₂ exchange. In high-risk cases, healthcare providers may recommend additional interventions, such as supplemental oxygen or closer monitoring of fetal acid-base balance. By understanding and supporting the placenta’s role in waste elimination, caregivers can safeguard fetal well-being and promote a healthy pregnancy.
Texting iPhones: Does It Waste SMS Money or Save Costs?
You may want to see also
Explore related products






![]()
Impact of placental dysfunction on fetal waste accumulation
The placenta, often referred to as the fetus's lifeline, plays a critical role in waste removal, ensuring the developing baby remains in a toxin-free environment. It efficiently filters out carbon dioxide, urea, and other metabolic byproducts, exchanging them for oxygen and nutrients from the mother's bloodstream. However, when placental dysfunction occurs, this delicate balance is disrupted, leading to a dangerous accumulation of waste products in the fetal system. This dysfunction can manifest in various ways, from reduced blood flow to improper nutrient and waste exchange, each with profound implications for fetal health.
Consider the case of placental insufficiency, a condition where the placenta fails to deliver adequate oxygen and nutrients to the fetus. As blood flow diminishes, the removal of waste products like carbon dioxide and urea becomes compromised. For instance, elevated fetal serum urea levels, often exceeding 2.5 mmol/L, can indicate impaired waste clearance. This buildup not only stresses the fetal kidneys but also contributes to intrauterine growth restriction (IUGR), where the baby’s weight falls below the 10th percentile for gestational age. Such scenarios underscore the placenta’s indispensable role in maintaining fetal homeostasis.
From a practical standpoint, monitoring placental function is crucial for early detection of waste accumulation. Ultrasound assessments of umbilical artery Doppler flow, amniotic fluid index, and fetal biophysical profiles can provide critical insights. For example, a pulsatility index (PI) above 95th percentile in the umbilical artery suggests increased resistance and reduced placental perfusion, a red flag for potential waste buildup. Healthcare providers should also track maternal symptoms like decreased fetal movement or sudden weight gain, which may signal placental dysfunction. Timely interventions, such as increased maternal hydration or low-dose aspirin in cases of suspected preeclampsia, can mitigate risks.
Comparatively, placental dysfunction’s impact on fetal waste accumulation is akin to a clogged filter in a water system—toxic byproducts linger, poisoning the environment. Unlike adults, fetuses lack fully developed organs to compensate for waste removal, making them entirely dependent on the placenta. When this system fails, the consequences are dire: acidosis from excess carbon dioxide, uremia from urea buildup, and long-term developmental delays. Studies show that fetuses with prolonged exposure to high waste levels are at increased risk of neurological impairments, with up to 30% exhibiting cognitive deficits by age 2.
In conclusion, placental dysfunction disrupts the fetus’s waste removal mechanism, leading to a cascade of adverse effects. From IUGR to long-term developmental issues, the implications are severe and often irreversible. Proactive monitoring, early intervention, and a deep understanding of placental physiology are essential to safeguarding fetal health. By treating placental dysfunction as a critical concern, healthcare providers can prevent waste accumulation and ensure a healthier start for newborns.
Save the Dates: Worth the Cost or Wasteful Wedding Expense?
You may want to see also
Frequently asked questions
Yes, the placenta plays a crucial role in removing waste products, such as carbon dioxide and urea, from the fetal bloodstream and transferring them to the maternal circulation for elimination.
The placenta eliminates fetal waste through a process called countercurrent exchange. Waste products from the fetus diffuse across the placental membrane into the maternal blood, where they are carried to the mother’s kidneys and lungs for excretion.
If the placenta fails to remove waste products effectively, it can lead to fetal distress, growth restrictions, or even life-threatening conditions such as fetal acidosis, as waste buildup can disrupt the fetus’s metabolic balance.