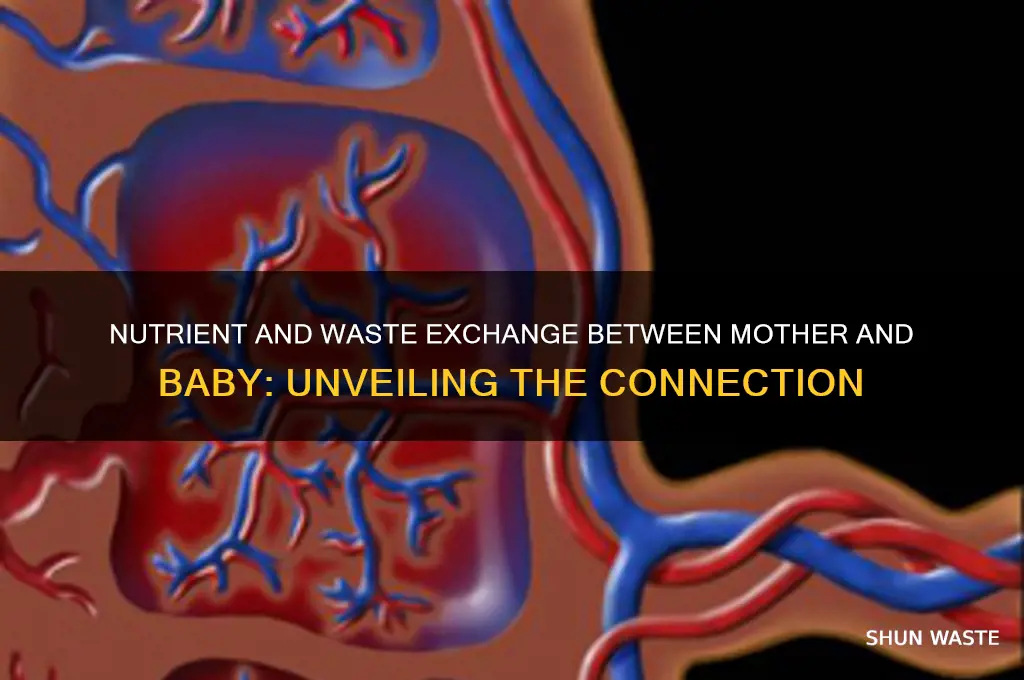
The relationship between a mother and her baby during pregnancy is a complex and fascinating process, involving a unique exchange of nutrients and waste products across the placenta. This vital organ acts as a bridge, allowing essential nutrients such as oxygen, glucose, and amino acids to pass from the mother's bloodstream to the developing fetus, while also facilitating the removal of waste products like carbon dioxide and urea. This intricate exchange is crucial for the baby's growth and development, as it relies entirely on the mother for sustenance and waste elimination. Understanding this process not only highlights the remarkable adaptability of the human body but also underscores the importance of maternal health in ensuring the well-being of the unborn child.
| Characteristics | Values |
|---|---|
| Exchange of Nutrients | Yes, the mother and fetus exchange nutrients via the placenta. Essential nutrients like glucose, amino acids, and fatty acids are transported from the mother's bloodstream to the fetus through the placental barrier. |
| Exchange of Oxygen | Yes, oxygen is transferred from the mother's bloodstream to the fetus via the placenta, supporting fetal growth and development. |
| Exchange of Waste Products | Yes, fetal waste products such as carbon dioxide and urea are transferred from the fetus to the mother through the placenta and then eliminated by the mother's kidneys and lungs. |
| Placental Barrier Function | The placenta acts as a selective barrier, allowing the exchange of nutrients, oxygen, and waste while preventing the passage of most harmful substances (e.g., bacteria, viruses) and large molecules. |
| Hormonal Regulation | The placenta produces hormones (e.g., human placental lactogen, progesterone) that regulate nutrient metabolism in both the mother and fetus, ensuring adequate nutrient supply. |
| Immune Protection | The placenta provides some immune protection to the fetus by limiting the transfer of maternal immune cells, though certain antibodies (IgG) can cross to provide passive immunity. |
| Nutrient Prioritization | In cases of maternal nutrient deficiency, the fetus is often prioritized, which can lead to maternal depletion of essential nutrients. |
| Waste Elimination Pathway | Fetal waste is primarily eliminated through the mother's renal and respiratory systems, as the fetus does not have functional kidneys or lungs for independent waste removal. |
| Impact of Maternal Diet | The quality of the mother's diet directly affects nutrient availability for the fetus, emphasizing the importance of adequate maternal nutrition during pregnancy. |
| Exchange Mechanism | Nutrient and waste exchange occurs via passive diffusion, facilitated transport, and active transport across the placental membrane. |
Explore related products






What You'll Learn
![]()
Placental nutrient transfer mechanisms
The placenta is a remarkable organ that facilitates the exchange of nutrients, gases, and waste products between the mother and the developing fetus. At its core, the placental nutrient transfer mechanisms are a complex interplay of passive and active processes, ensuring the growing baby receives essential nutrients while eliminating waste efficiently. These mechanisms are critical for fetal growth and development, making the placenta a lifeline for the unborn child.
Passive Diffusion: The Unregulated Exchange
One of the primary mechanisms of nutrient transfer is passive diffusion, which relies on concentration gradients. Small molecules like glucose, amino acids, and oxygen move freely from the maternal bloodstream to the fetal circulation through the placental barrier. For instance, glucose, a vital energy source for the fetus, diffuses across the placenta until its concentration in fetal blood matches that of the mother. However, this process is not without limitations. Larger molecules, such as intact proteins and insulin, cannot pass through, necessitating alternative pathways. Pregnant women are often advised to maintain stable blood sugar levels, as fluctuations directly impact fetal glucose availability, potentially affecting growth and development.
Active Transport: The Regulated Supply
Unlike passive diffusion, active transport requires energy and is highly regulated. This mechanism ensures the fetus receives essential nutrients, even when maternal levels are low. For example, calcium and iron are transported actively across the placenta, driven by specific carrier proteins. The fetus requires approximately 30 mg of iron daily during the third trimester, a demand met through this active process. Similarly, amino acids, the building blocks of proteins, are transported actively to support rapid fetal tissue growth. This regulated system prioritizes fetal needs, often at the expense of maternal reserves, highlighting the placenta’s role in safeguarding the baby’s development.
Endocytosis and Exocytosis: The Bulk Movement
For larger molecules that cannot diffuse or be actively transported, the placenta employs endocytosis and exocytosis. These processes involve the engulfing and release of substances in vesicles. Immunoglobulin G (IgG), a critical antibody for fetal immune protection, is transferred via this mechanism. Starting around 13 weeks of gestation, IgG is endocytosed from the maternal blood, transported across placental cells, and exocytosed into the fetal circulation. This ensures the fetus receives passive immunity, protecting it from infections during the first few months of life. While efficient, this process is selective, as not all maternal antibodies can cross the placenta.
Waste Removal: A Reverse Journey
Just as nutrients are transferred to the fetus, waste products like urea and carbon dioxide are removed. This occurs primarily through passive diffusion, as these waste molecules move from the fetal bloodstream, where their concentration is higher, to the maternal circulation. The mother’s kidneys and lungs then eliminate these wastes. This reverse exchange is essential, as the fetus lacks fully developed excretory systems. For example, fetal urea, a byproduct of protein metabolism, is continuously shunted to the mother, preventing its accumulation in the fetal environment.
Understanding placental nutrient transfer mechanisms underscores the placenta’s role as a dynamic interface, balancing the needs of both mother and fetus. From passive diffusion to active transport and bulk movement, these processes ensure the fetus receives vital nutrients while waste is efficiently removed. Pregnant women can support these mechanisms by maintaining a balanced diet rich in essential nutrients like iron, calcium, and protein, and by monitoring conditions like gestational diabetes that disrupt glucose transfer. The placenta’s intricate design highlights the precision of nature in fostering life.
AC Fan Energy Usage: Is It Draining Your Power Bill?
You may want to see also
Explore related products






![]()
Waste removal pathways in utero
The placenta, a temporary organ connecting mother and fetus, serves as the primary waste removal system in utero. Fetal waste products, primarily carbon dioxide, urea, and creatinine, diffuse across the placental membrane into the maternal bloodstream. This passive process relies on the concentration gradient between fetal and maternal blood, ensuring efficient waste elimination without requiring active energy expenditure from the fetus.
Understanding this mechanism highlights the placenta's dual role as both a nutrient provider and a waste disposal unit, crucial for fetal development and well-being.
Imagine a sophisticated filtration system, constantly working to maintain a healthy environment for the growing fetus. The placenta acts as a selective barrier, allowing essential nutrients and oxygen to pass from mother to baby while effectively blocking harmful substances. This intricate process involves specialized cells and transport mechanisms. For instance, glucose, a vital energy source, is actively transported against its concentration gradient, ensuring a steady supply for the developing fetus. Conversely, waste products like urea, a byproduct of protein metabolism, freely diffuse from the fetus into the maternal circulation, where they are ultimately eliminated through the mother's kidneys.
This intricate dance of molecules across the placental barrier is a testament to the remarkable adaptability of the human body during pregnancy.
While the placenta handles the majority of waste removal, the fetal urinary system also plays a role. Fetal urine, produced by the developing kidneys, is expelled into the amniotic fluid surrounding the baby. This fluid, swallowed by the fetus, is then reabsorbed, creating a closed loop system. Interestingly, components of fetal urine, such as urea, can also diffuse across the amniotic membrane into the maternal circulation, providing an additional pathway for waste elimination. This dual waste removal system underscores the redundancy built into fetal development, ensuring the baby's environment remains optimal even if one pathway is compromised.
Understanding waste removal pathways in utero has practical implications for prenatal care. Monitoring amniotic fluid volume and composition can provide valuable insights into fetal health. For example, decreased amniotic fluid levels or abnormal concentrations of waste products may indicate potential issues with placental function or fetal well-being. Additionally, certain maternal conditions, such as diabetes, can affect waste removal efficiency, highlighting the importance of managing maternal health for optimal fetal development. By recognizing the intricate waste removal processes at play, healthcare providers can better assess fetal health and intervene when necessary, ensuring a healthy start for both mother and baby.
Applied Fluid Power Automation: Streamlining Efficiency and Reducing Waste
You may want to see also
Explore related products






![]()
Maternal-fetal nutrient sharing dynamics
During pregnancy, the placenta acts as a dynamic interface where maternal-fetal nutrient sharing occurs, ensuring the growing fetus receives essential elements for development while eliminating waste products. This process is highly regulated, with specific transport mechanisms facilitating the exchange of nutrients like glucose, amino acids, and lipids, which are critical for fetal growth. For instance, glucose crosses the placenta via facilitated diffusion, with maternal glucose levels directly influencing fetal supply. However, this system is not without limitations; excessive maternal glucose can lead to fetal macrosomia, highlighting the delicate balance required in nutrient transfer.
Consider the role of amino acids, which are vital for fetal protein synthesis and organ development. The placenta prioritizes their transfer through active transport systems, ensuring a steady supply even when maternal levels fluctuate. Studies show that maternal protein intake of at least 70 grams daily supports optimal fetal amino acid availability, particularly during the third trimester when demands peak. Conversely, maternal deficiencies can impair fetal growth, emphasizing the interdependence of maternal and fetal nutrition.
Waste removal is equally critical in this exchange. Urea, a byproduct of fetal protein metabolism, is transported back to the maternal circulation for renal excretion. This process relies on the placenta’s ability to act as a selective barrier, preventing the accumulation of toxic substances in the fetal environment. However, certain waste products, like bilirubin, are not efficiently cleared, necessitating fetal liver development to manage these compounds. This dual function of nutrient provision and waste elimination underscores the placenta’s complexity as a life-sustaining organ.
Practical considerations for optimizing maternal-fetal nutrient sharing include monitoring maternal diet and health. For example, maintaining a balanced intake of macronutrients (carbohydrates, proteins, and fats) ensures adequate nutrient availability for the fetus. Additionally, managing conditions like gestational diabetes is crucial, as uncontrolled blood sugar levels can disrupt glucose transfer dynamics. Prenatal supplements, particularly folic acid (400–600 mcg daily) and iron (27 mg daily), are recommended to address increased fetal demands and prevent deficiencies that could compromise development.
In summary, maternal-fetal nutrient sharing dynamics are a finely tuned process that supports fetal growth while managing waste. Understanding this interplay allows for targeted interventions to enhance pregnancy outcomes. By focusing on maternal nutrition, health, and placental function, healthcare providers and expectant mothers can collaboratively ensure a healthy developmental environment for the fetus. This knowledge transforms pregnancy care from a passive observation of growth to an active optimization of nutrient exchange.
Efficient Metabolic Waste Removal: Insights from Laboratory Studies
You may want to see also
Explore related products






![]()
Impact of maternal diet on fetal nutrients
The placenta acts as a selective gatekeeper, facilitating the exchange of nutrients and waste between mother and fetus. This intricate process is heavily influenced by the maternal diet, which directly impacts the quality and quantity of nutrients available to the developing baby. Essential nutrients like folate, iron, calcium, and omega-3 fatty acids are particularly critical during pregnancy, as deficiencies can lead to severe fetal complications. For instance, inadequate folate intake increases the risk of neural tube defects, while insufficient iron can result in fetal anemia and low birth weight.
Consider the role of macronutrients: proteins, carbohydrates, and fats. A balanced intake ensures proper fetal growth and development. Pregnant women require an additional 25 grams of protein daily to support tissue synthesis in the fetus. Carbohydrates, preferably complex ones like whole grains, provide sustained energy for both mother and baby, while healthy fats, such as those found in avocados and nuts, are vital for brain and nervous system development. However, excessive consumption of processed sugars and saturated fats can lead to gestational diabetes and macrosomia (excessive birth weight), highlighting the need for moderation and mindful eating.
Micronutrients, though needed in smaller amounts, are equally indispensable. Vitamin D, for example, is crucial for bone health and immune function in the fetus. Pregnant women are often advised to take 600 IU of vitamin D daily, as deficiency is common and linked to preeclampsia and low birth weight. Similarly, iodine is essential for thyroid function and cognitive development, with a recommended intake of 220 mcg daily during pregnancy. Practical tips include incorporating fortified foods like dairy products and seafood into the diet, while avoiding excessive caffeine and unpasteurized items that can interfere with nutrient absorption.
The timing and consistency of nutrient intake also matter. Early pregnancy is a critical period for organogenesis, making adequate nutrition during the first trimester paramount. For example, folic acid supplementation (400–800 mcg daily) should ideally begin before conception and continue through the first 12 weeks to prevent neural tube defects. Later in pregnancy, calcium requirements increase to 1,000–1,300 mg daily to support fetal bone development. A well-structured meal plan, including frequent, nutrient-dense snacks, can help maintain stable blood sugar levels and ensure a steady supply of nutrients to the fetus.
In conclusion, the maternal diet is a cornerstone of fetal health, shaping growth, development, and long-term outcomes. By prioritizing a balanced intake of macronutrients and micronutrients, pregnant women can optimize the nutrient exchange across the placenta. Practical steps, such as supplementation, mindful food choices, and consistent meal planning, empower mothers to nurture their babies from the earliest stages of life. This proactive approach not only safeguards fetal well-being but also lays the foundation for lifelong health.
Does Sam's Club Offer Yard Waste Bags? A Quick Guide
You may want to see also
Explore related products





![]()
Fetal waste excretion and maternal processing
The fetus, despite its remarkable development, lacks the fully functional organs needed for independent waste management. This critical task falls to the mother, whose body acts as a sophisticated filtration system for the growing life within. Fetal waste products, primarily urea, carbon dioxide, and creatinine, are transferred across the placenta into the maternal bloodstream. The mother's kidneys then filter these waste products, which are eventually excreted through her urine. This process highlights the intricate interdependence between mother and fetus, where the mother's organs effectively serve as a surrogate waste disposal system.
Understanding this mechanism is crucial for prenatal care. For instance, maternal kidney function must be closely monitored, as any impairment can lead to a buildup of fetal waste products, potentially harming the developing baby. Conditions like preeclampsia, characterized by high blood pressure and kidney dysfunction, underscore the delicate balance required for this waste exchange system to function optimally.
Consider the placenta as a highly selective gatekeeper, allowing essential nutrients to pass from mother to fetus while simultaneously permitting fetal waste to exit. This dual functionality is a testament to the placenta's complexity. It ensures that the fetus receives the necessary building blocks for growth while preventing the accumulation of harmful byproducts. However, this system is not without its vulnerabilities. Certain maternal conditions, such as diabetes or infections, can compromise placental function, disrupting the efficient exchange of nutrients and waste. This disruption can lead to fetal growth restrictions or other developmental issues, emphasizing the need for comprehensive maternal health management during pregnancy.
From a practical standpoint, pregnant women can support this vital waste processing system through simple yet effective measures. Staying well-hydrated is paramount, as it aids in kidney function and facilitates the elimination of waste products. A balanced diet rich in fruits, vegetables, and whole grains provides essential nutrients while minimizing the intake of processed foods that can burden the system. Regular prenatal check-ups are essential to monitor both maternal and fetal health, allowing for early detection and management of any potential issues. By adopting these practices, mothers can actively contribute to the efficient processing of fetal waste, fostering a healthier environment for their developing baby.
In conclusion, fetal waste excretion and maternal processing are integral components of the nutrient and waste exchange between mother and baby. This symbiotic relationship relies on the placenta's functionality and the mother's organs, particularly her kidneys. Awareness of this process and its potential challenges empowers both healthcare providers and expectant mothers to take proactive steps in ensuring a healthy pregnancy. Through proper care and monitoring, the intricate dance of nutrient and waste exchange can proceed smoothly, laying the foundation for a thriving newborn.
Placental Exchange: Nutrients, Gases, and Waste Transport Across the Placenta
You may want to see also
Frequently asked questions
Yes, the mother and baby exchange nutrients through the placenta. The mother’s blood supplies oxygen and nutrients like glucose, amino acids, and fatty acids to the baby via the placenta, which the baby uses for growth and development.
The baby does not directly receive waste products from the mother. Instead, the baby produces its own waste (like carbon dioxide and urea), which is transferred to the mother’s bloodstream through the placenta. The mother’s kidneys and lungs then eliminate these waste products.
Yes, the mother’s diet directly impacts the baby’s nutrient intake. A balanced diet rich in essential nutrients ensures the baby receives adequate nourishment. Poor maternal nutrition can lead to deficiencies in the baby.
The baby produces its own waste products, such as carbon dioxide and urea, from its metabolic processes. These waste products are transferred to the mother’s bloodstream through the placenta, and the mother’s body eliminates them via her kidneys, lungs, and other excretory systems.
Yes, disruptions in nutrient or waste exchange can lead to serious complications. Poor nutrient transfer may result in fetal growth restriction or malnutrition, while inefficient waste removal can cause fetal toxicity or distress. Conditions like placental insufficiency can impair this exchange.





























