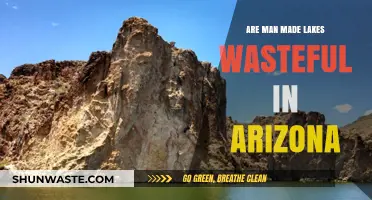
Loop diuretics, commonly prescribed for conditions like hypertension and heart failure, are known for their potent diuretic effects by inhibiting the Na-K-2Cl cotransporter in the thick ascending loop of Henle. However, a critical consideration in their use is their impact on potassium levels. Unlike potassium-sparing diuretics, which preserve or increase serum potassium, loop diuretics are classified as potassium-wasting diuretics. This is because they promote significant sodium and chloride excretion, which indirectly leads to increased potassium loss through enhanced distal tubular delivery of sodium and aldosterone-mediated potassium secretion. As a result, patients on loop diuretics often require potassium supplementation or concurrent use of potassium-sparing agents to mitigate the risk of hypokalemia. Understanding this distinction is essential for safe and effective management of fluid and electrolyte balance in clinical practice.
| Characteristics | Values |
|---|---|
| Potassium Effect | Wasting (cause significant potassium loss) |
| Mechanism of Action | Inhibit Na+/K+/2Cl- cotransporter in the thick ascending limb of Henle |
| Examples | Furosemide, Bumetanide, Torsemide |
| Primary Use | Treatment of edema, hypertension, and heart failure |
| Potassium Monitoring | Regular monitoring required; supplementation often necessary |
| Common Side Effects | Hypokalemia, dehydration, ototoxicity, electrolyte imbalances |
| Onset of Action | Rapid (within 30 minutes to 1 hour) |
| Duration of Action | 2-3 hours (furosemide), up to 6 hours (torsemide) |
| Contraindications | Anuria, severe electrolyte imbalances, hypersensitivity |
| Pregnancy Category | B (furosemide, bumetanide), C (torsemide) |
| Excretion | Primarily renal |
| Drug Interactions | Potentiates effects of antihypertensives, increases ototoxicity with aminoglycosides |
| Special Populations | Caution in elderly, renal impairment, and diabetes |
| Alternative Potassium-Sparing Diuretics | Spironolactone, Triamterene, Amiloride (spare potassium) |
Explore related products






What You'll Learn
![]()
Mechanism of loop diuretics on potassium excretion
Loop diuretics, such as furosemide and torsemide, are widely prescribed for conditions like hypertension and heart failure due to their potent ability to increase urine output. However, their impact on potassium excretion is a critical consideration for clinicians and patients alike. These medications act primarily on the thick ascending limb of the loop of Henle in the kidney, inhibiting the sodium-potassium-chloride cotransporter (NKCC2). This mechanism disrupts the reabsorption of sodium and chloride, leading to increased urinary excretion of these ions. Potassium, though not directly transported by NKCC2, is indirectly affected due to alterations in the electrochemical gradient and increased distal delivery of sodium, which enhances potassium secretion in the distal tubule and collecting duct.
The net effect of loop diuretics on potassium levels is typically wasting, meaning they promote potassium loss. For instance, a standard dose of furosemide (40–80 mg daily) can lead to a significant decrease in serum potassium, particularly in patients with pre-existing hypokalemia or those on concurrent medications that further deplete potassium. Elderly patients and individuals with chronic kidney disease are especially vulnerable due to reduced renal reserve and altered electrolyte handling. Monitoring serum potassium levels is essential, with adjustments made through dietary potassium supplementation (e.g., bananas, oranges, or spinach) or potassium-sparing diuretics like spironolactone if levels drop below 3.5 mmol/L.
To mitigate potassium wasting, clinicians often employ a stepwise approach. First, assess baseline potassium levels and renal function before initiating loop diuretic therapy. Second, consider co-prescribing a potassium supplement or potassium-sparing diuretic, particularly in high-risk populations. For example, combining furosemide with spironolactone (25–50 mg daily) can help maintain potassium balance while enhancing diuretic efficacy. Third, educate patients on dietary sources of potassium and signs of hypokalemia, such as muscle weakness, fatigue, or arrhythmias, to ensure prompt intervention.
A comparative analysis highlights the contrast between loop diuretics and potassium-sparing diuretics like amiloride or triamterene, which directly inhibit sodium reabsorption in the distal tubule without promoting potassium loss. While loop diuretics are more effective for acute volume overload, their potassium-wasting effects necessitate careful management. In contrast, potassium-sparing agents are often reserved for milder cases or as adjuncts to loop diuretics. Understanding these differences allows for tailored therapy that balances diuresis with electrolyte stability, ensuring optimal patient outcomes.
In summary, loop diuretics are inherently potassium-wasting due to their mechanism of action, which increases distal sodium delivery and potassium secretion. Practical strategies, including monitoring, supplementation, and combination therapy, are essential to counteract this effect. By integrating these measures, clinicians can harness the therapeutic benefits of loop diuretics while minimizing the risk of hypokalemia, particularly in vulnerable populations. This nuanced approach underscores the importance of individualized care in managing complex conditions like heart failure and hypertension.
Lymphatic System and Kidney Waste: Unraveling the Connection
You may want to see also
Explore related products





![]()
Comparison with potassium-sparing diuretics
Loop diuretics, such as furosemide and torsemide, are known for their potent ability to increase urine output by inhibiting the Na-K-2Cl cotransporter in the thick ascending limb of the loop of Henle. This mechanism, while effective in managing conditions like hypertension and heart failure, leads to significant potassium loss, often requiring supplementation or additional medication to prevent hypokalemia. In contrast, potassium-sparing diuretics, including spironolactone and eplerenone, act on the distal tubule and collecting duct, blocking aldosterone receptors and minimizing potassium excretion. This fundamental difference in action highlights the need for a nuanced comparison when choosing between these classes.
When prescribing diuretics, clinicians must consider the patient’s potassium status and comorbidities. For instance, loop diuretics are often the first-line choice for acute decompensated heart failure due to their rapid onset and high efficacy, but their potassium-wasting effects necessitate monitoring. A typical starting dose of furosemide is 20–40 mg/day, which can be titrated up to 160 mg/day in severe cases. However, in patients with chronic kidney disease or those on concurrent medications that lower potassium, the risk of hypokalemia escalates, making potassium-sparing diuretics a safer alternative. Spironolactone, for example, is commonly dosed at 25–50 mg/day in heart failure patients, offering both diuresis and potassium conservation.
The combination of loop diuretics with potassium-sparing agents is a strategic approach to maximize fluid removal while mitigating potassium loss. For example, a patient on 80 mg of furosemide daily might be prescribed 25 mg of spironolactone to counteract potassium depletion. This combination is particularly useful in elderly patients or those with diabetes, who are at higher risk for electrolyte imbalances. However, caution is advised in patients with renal impairment, as potassium-sparing diuretics can lead to hyperkalemia if renal function is severely compromised. Regular serum potassium checks, ideally every 1–2 weeks after initiating therapy, are essential to ensure safety.
From a practical standpoint, patient education plays a critical role in managing diuretic therapy. Individuals on loop diuretics should be advised to consume potassium-rich foods like bananas, oranges, and spinach, but this alone may not suffice, especially at higher diuretic doses. Potassium supplements, such as 10–20 mEq daily, may be necessary under medical supervision. Conversely, patients on potassium-sparing diuretics should avoid excessive potassium intake and be warned about symptoms of hyperkalemia, such as muscle weakness or irregular heartbeat. This dual focus on dietary habits and medication adherence ensures a balanced approach to diuretic therapy.
In summary, while loop diuretics are indispensable for their rapid and robust diuretic effects, their potassium-wasting nature demands careful management. Potassium-sparing diuretics offer a complementary solution, particularly in high-risk populations, but require vigilant monitoring to avoid hyperkalemia. By understanding the distinct mechanisms and clinical implications of these classes, healthcare providers can tailor therapy to individual patient needs, optimizing outcomes while minimizing risks.
Republic Services and Waste Management: Acquisition Rumors Explained
You may want to see also
Explore related products






![]()
Clinical effects on serum potassium levels
Loop diuretics, such as furosemide and torsemide, are known for their potent diuretic effects, primarily acting on the thick ascending limb of the loop of Henle to increase sodium and chloride excretion. However, their impact on serum potassium levels is a critical clinical consideration. These agents are classified as potassium-wasting diuretics, meaning they promote significant potassium loss through urinary excretion. This effect is dose-dependent; higher doses of loop diuretics (e.g., furosemide > 40 mg/day) are more likely to cause hypokalemia, particularly in patients with heart failure, cirrhosis, or chronic kidney disease. Monitoring serum potassium levels is essential, especially in older adults and those on concurrent medications that further lower potassium, such as corticosteroids or amphotericin B.
The mechanism behind potassium wasting with loop diuretics involves increased distal sodium delivery, which enhances potassium secretion in the distal tubule. This process is further exacerbated by the activation of the renin-angiotensin-aldosterone system (RAAS), which promotes potassium excretion in exchange for sodium reabsorption. Clinically, hypokalemia can manifest as muscle weakness, arrhythmias, or gastrointestinal symptoms, requiring prompt intervention. To mitigate this risk, potassium supplementation (oral or intravenous) or co-prescription of potassium-sparing diuretics like spironolactone may be necessary, particularly in patients with baseline potassium levels below 4.0 mmol/L.
In contrast to loop diuretics, potassium-sparing diuretics (e.g., spironolactone, eplerenone) directly antagonize aldosterone, reducing potassium excretion and often raising serum potassium levels. When combining loop diuretics with potassium-sparing agents, clinicians must carefully balance the need for diuresis with the risk of hyperkalemia, especially in patients with renal impairment or diabetes. Regular monitoring of serum potassium and renal function is crucial in such cases, with adjustments made based on levels (e.g., target potassium 4.0–5.0 mmol/L).
Practical tips for managing potassium levels in patients on loop diuretics include encouraging dietary potassium intake (e.g., bananas, oranges, spinach) unless contraindicated, and educating patients about symptoms of hypo- or hyperkalemia. For those on high-dose loop diuretics, starting with a low-dose potassium supplement (e.g., 10–20 mEq/day) and titrating based on serum levels is a prudent strategy. In urgent cases of severe hypokalemia (e.g., < 3.0 mmol/L with ECG changes), intravenous potassium replacement (e.g., 10–20 mEq/hour) under cardiac monitoring is warranted.
In summary, loop diuretics are potassium-wasting agents with significant clinical implications for serum potassium levels. Their use requires vigilant monitoring, particularly in high-risk populations, and often necessitates adjunctive strategies to maintain potassium homeostasis. Understanding these effects is essential for safe and effective diuretic therapy.
How the Small Intestine Eliminates Waste: A Digestive Journey
You may want to see also
Explore related products






![]()
Risk of hypokalemia with loop diuretics
Loop diuretics, such as furosemide and torsemide, are potent medications primarily used to treat hypertension and edema associated with heart failure, liver disease, and kidney disorders. While their efficacy in promoting diuresis is well-established, a critical side effect demands attention: these drugs are potassium-wasting, significantly increasing the risk of hypokalemia. This occurs because loop diuretics inhibit the Na-K-2Cl cotransporter in the thick ascending limb of the loop of Henle, leading to excessive renal excretion of both sodium and chloride, with potassium following suit to maintain electrical neutrality. Unlike potassium-sparing diuretics, which directly or indirectly preserve potassium levels, loop diuretics deplete potassium stores, often requiring proactive management to prevent complications.
The risk of hypokalemia with loop diuretics is dose-dependent, with higher doses exacerbating potassium loss. For instance, furosemide doses exceeding 80 mg/day are particularly associated with severe hypokalemia, especially in elderly patients or those with pre-existing renal impairment. Hypokalemia can manifest as muscle weakness, fatigue, arrhythmias, or even life-threatening cardiac complications, such as torsades de pointes. Monitoring serum potassium levels is essential, particularly during the initial weeks of therapy or after dosage adjustments. Patients should be educated to recognize symptoms of hypokalemia and report them promptly to their healthcare provider.
To mitigate the risk, clinicians often prescribe potassium supplementation or potassium-sparing diuretics (e.g., spironolactone or amiloride) alongside loop diuretics. For example, a patient on 40 mg of furosemide daily might be advised to take 10–20 mEq of oral potassium chloride daily, depending on their baseline potassium levels. Dietary modifications, such as increasing intake of potassium-rich foods like bananas, oranges, spinach, and potatoes, can complement pharmacological interventions. However, caution is warranted in patients with chronic kidney disease or those on angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), as excessive potassium supplementation can lead to hyperkalemia.
Practical tips for patients include consistent monitoring of potassium levels, adherence to prescribed dosages, and avoiding over-the-counter medications that may exacerbate potassium loss, such as nonsteroidal anti-inflammatory drugs (NSAIDs). For elderly patients or those with cognitive impairments, caregivers should ensure medication compliance and dietary adjustments. Regular follow-ups with healthcare providers are crucial to assess electrolyte balance and adjust therapy as needed. By understanding the potassium-wasting nature of loop diuretics and implementing proactive measures, the risk of hypokalemia can be effectively managed, ensuring safer and more effective treatment outcomes.
Navigating to Maguuma Wastes in Guild Wars 2: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Strategies to manage potassium loss
Loop diuretics, such as furosemide and torsemide, are known to be potassium-wasting, meaning they increase urinary excretion of potassium and can lead to hypokalemia if not managed properly. This effect is particularly significant in patients with heart failure, hypertension, or chronic kidney disease who rely on these medications for fluid management. To counteract potassium loss, a multifaceted approach is essential, combining dietary adjustments, medication strategies, and regular monitoring.
Dietary Modifications: The Foundation of Potassium Balance
Incorporating potassium-rich foods into the diet is the first line of defense against hypokalemia. Foods like bananas (422 mg per medium banana), spinach (839 mg per cooked cup), sweet potatoes (542 mg per medium potato), and avocados (690 mg per avocado) are excellent sources. For older adults or those with reduced appetite, potassium-fortified beverages or supplements may be considered, but only under medical supervision to avoid hyperkalemia. A daily intake of 3,500–4,700 mg of potassium is generally recommended for adults, but individual needs vary based on diuretic dosage and renal function.
Medication Strategies: Spironolactone and Beyond
Adding a potassium-sparing diuretic, such as spironolactone or eplerenone, can mitigate potassium loss while maintaining diuretic efficacy. Spironolactone, typically dosed at 25–50 mg daily, is particularly effective in heart failure patients, reducing both hypokalemia and mortality. Alternatively, potassium-sparing agents like amiloride (5–10 mg daily) or triamterene (50–100 mg daily) can be paired with loop diuretics. However, these combinations require careful monitoring, especially in patients with renal impairment, as they may increase the risk of hyperkalemia.
Potassium Supplementation: Dosage and Cautions
Oral potassium supplements (e.g., chloride or citrate) are often prescribed when dietary intake is insufficient. Doses range from 10–40 mEq daily, divided to minimize gastrointestinal side effects. Extended-release formulations are preferred to reduce peak potassium levels. Patients with advanced chronic kidney disease (eGFR <30 mL/min/1.73 m²) or those taking ACE inhibitors or ARBs should avoid supplements unless closely monitored, as these factors increase hyperkalemia risk.
Monitoring and Adjustments: The Key to Safety
Regular serum potassium monitoring is critical, especially during the initial weeks of diuretic therapy or dosage adjustments. For high-risk patients, weekly checks may be necessary until stability is achieved. Symptoms of hypokalemia, such as muscle weakness, arrhythmias, or fatigue, warrant immediate medical attention. Conversely, signs of hyperkalemia, including palpitations or paresthesias, require prompt intervention, such as reducing potassium intake or discontinuing supplements.
By combining dietary potassium, strategic medication use, and vigilant monitoring, healthcare providers can effectively manage potassium loss associated with loop diuretics. This approach ensures patients receive the fluid-lowering benefits of these medications without compromising electrolyte balance or cardiovascular safety.
Unseen Losses: How Power Stations Waste Energy and Solutions
You may want to see also
Frequently asked questions
Loop diuretics are potassium wasting, meaning they increase the excretion of potassium in the urine, which can lead to hypokalemia (low potassium levels) if not managed properly.
Loop diuretics, such as furosemide, work by inhibiting the sodium-potassium-chloride cotransporter in the thick ascending limb of the loop of Henle, leading to increased excretion of sodium, chloride, and potassium in the urine, thereby causing potassium depletion.
Yes, potassium supplementation, either through diet or supplements, or the concurrent use of potassium-sparing diuretics (e.g., spironolactone, amiloride) can help mitigate the potassium wasting effects of loop diuretics and maintain normal potassium levels in the body. However, close monitoring of potassium levels is essential to avoid hyperkalemia (high potassium levels).